

Short-term Usual Chiropractic Care for Spinal Pain:
A Randomized Controlled TrialThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Spine (Phila Pa 1976). 2013 (Nov 15); 38 (24): 2071–2078 ~ FULL TEXT
Bruce F. Walker, DC, MPH, DrPH, Jeff J. Hebert, DC, PhD, Norman J. Stomski, PhD, Barrett Losco, MChiropractic, and Simon D. French, PhD
School of Health Professions
School of Psychology and Exercise Science,
Murdoch University,
Murdoch, Australia; and
School of Rehabilitation Therapy,
Queen's University,
Kingston, Ontario, Canada.

STUDY DESIGN: Parallel-group randomized controlled trial.
OBJECTIVE: Establish the short-term effectiveness of chiropractic therapy for spinal pain compared with a sham intervention and explore the predictors of chiropractic treatment satisfaction.
SUMMARY OF BACKGROUND DATA: Chiropractic treatment is widely used for spinal pain. However, a lack of sound evidence precludes conclusions about the effectiveness of chiropractic for spinal pain.
METHODS: Participants were adults experiencing spinal pain, randomized to receive 2 treatments of chiropractic or sham therapy. Participants and outcome assessors were blinded to group allocation. Primary outcomes at 2 weeks were pain intensity (0–10 scale) and function (0–40 Functional Rating Index). Secondary outcomes were global change, minimum acceptable outcome, and treatment satisfaction. Treatment effects were estimated with linear mixed models for the primary outcomes. We used logistic regression to identify differences in the secondary outcomes and explore for predictors of treatment satisfaction.
RESULTS: One hundred eighty three participants (chiropractic, n = 92; sham, n = 91) were recruited and included in the analyses. Participants receiving chiropractic therapy reported greater improvements in pain (mean difference, 95% confidence interval [CI] = 0.5 [0.1–0.9]), physical function (mean difference [95% CI] = 2.1 [0.3–4.0]), and were more likely to experience global improvement (48% vs. 24%, P = 0.01) and treatment satisfaction (78% vs. 56%, P < 0.01). There was no between-group difference in achieving a minimally acceptable outcome (34% sham vs. 29% chiropractic, P = 0.42). Awareness of treatment assignment and achieving minimally important improvement in pain intensity were associated with chiropractic treatment satisfaction.
CONCLUSION: Short-term chiropractic treatment was superior to sham; however, treatment effects were not clinically important. Awareness of treatment assignment and clinically important reductions in pain were associated with chiropractic treatment satisfaction.
Key words: back pain, neck pain, effectiveness, chiropractic, manipulation, spinal, randomized controlled trial, clinical trial.
From the FULL TEXT Article:
Introduction
According to the 2010 Global Burden of Disease study, musculoskeletal disorders were the second leading kcause of disability throughout the worid. [1] In terms of individual disorders, the 2 most common forms of spinal pain, low back pain and neck pain, ranked respectively as the leading and fourth leading cause of disability-adjusted life years, [1]
This level of disability results in a substantial socioeconomic burden in both direct medical costs and indirect costs such as work absence and decreased productivity. [1–4] Hence, effective management of spinal pain is an important issue for patients, clnicians, and health care policy makers.
In high-income countries chiropractic treatment is widely used for spinal pain. [3, 5] However, recent systematic reviews have reported that small effect sizes of treatment and methodological limitations in published studies raise uncertainty about the value of chiropractic treatment. [6–9] A primary limitation of previous studies is the lack of randomized controlled trials comparing the effects of chiropractic treatment to inert interventions for spinal pain. [6–9]
Accordingly, our primary aim was to examine the comparative effectiveness of a brief chiropractic intervention compared with sham treatment for participants with spinal pain. The secondary aim was to explore the clinical and demographic variables associated with treatment satisfaction.
MATERIALS AND METHODS
Study Design
In this article, we report the secondary analysis of a 2–arm parallel-group randomized trial that compared the effectiveness of usual chiropractic treatment to a sham intervention. The primary analysis examined the occurrence of adverse events and this has been published elsewhere.'" The protocol for this trial was published and the trial was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12611000542998)." All data were collected during the 3 months between August 2012 and October 2012 in 12 Western Australian metropolitan chiropractic clinics.
Ethics
Ethics approval was obtained from Murdoch University's Human Research Committee (2011/109). The information letter provided to potential participants stated that the study will compare one type of chiropractic treatment that has unknown benefits for back pain with another type of chiropractic treatment that is not thought to be beneficial for back pain. These words were accepted by the Human Research Ethics Committee and written informed consent was obtained from all participants prior to inclusion in this study.
Recruitment and Eligibility Criteria
We recruited participants from the local community using newspaper advertisements. All included participants were 18 years or older; English literate; had current spinal pain (neck, midback, or low back pain) of at least 1–week duration; and scored at least 3 out of a maximum 10 on the Numerical Rating Scale (NRS) for pain, [12] and 12 out of a maximum 40 on the Functional Rating Index (FRI). [13]
Participants were excluded if they thought they would be unable to tolerate any intervention potentially provided in usual chiropractic care including: manipulative therapy, mobilization, traction, massage, ultrasound, and physical modalities. Participants were also excluded if they had: spinal pain related to cancer or infection, spinal fracture, spondyloarthropathy, known osteoporosis, progressive upper or lower limb weakness, symptoms of cauda equina syndrome or other significant neurological condition, recent disc herniation, known severe cardiovascular disease, uncontrolled hypertension, cognitive impairment, blood coagulation disorder, previous spinal surgery in the past year, previous history of stroke or transient ischémie attacks, pacemaker or other electrical device implanted, substance abuse issues, pregnancy, or a current compensation claim.
Interventions
Participants were assigned to either a sham group or a usual chiropractic care group, whereupon 2 treatments were provided with approximately 1–week between treatments. Chiropractors providing either the sham or usual chiropractic treatment attended a 3–hour training session in which the trial protocols were detailed and the administration of the sham intervention was demonstrated. Ongoing guidance was also provided to the chiropractors throughout the trial. To be eligible, all chiropractors were required to practice within the Western Australian metropolitan region of Perth and were registered with the Chiropractic Board of Australia.Sham Group Four chiropractors in this group delivered the following procedures at each visit
(1) detuned ultrasound [14];
(2) an Activator instrument (Activator Methods International, Ltd., Phoenix, AZ), [15] a hand held device that delivers a low impulse thrust, but was delivered at its lowest output and randomly administered on or around the spine through a tongue depressor to disperse any remaining force; and
(3) a randomly placed hand on the spine while the detuned ultrasound head was placed on the participant's back/neck to give a "hands on" experience. As part of their training, the 4 chiropractors were instructed to show equal enthusiasm for the sham therapy as they would for usual care.Usual Chiropractic Care Eight chiropractors in this group administered individualized chiropractic care in line with their usual treatment approach. All chiropractors were asked to adhere to Australian evidencebased guidelines for acute musculoskeletal pain regarding the use of imaging. [16]
Randomization
A random number generator was used to create a permuted block randomization list with variable block sizes of 8 to 12. Allocation was concealed with group assignment sealed in sequentially numbered, opaque envelopes. Staff not administering baseline or outcome measures opened the envelope and allocated eligible participants to 1 of the intervention groups.
Outcome Assessment
Staff administering baseline or outcome measures were blinded to group allocation. [17] For this effectiveness analysis, the primary outcomes were pain intensity, measured on an 11–point NRS and derived by averaging current, best, and worst pain intensity in the preceding 48 hours [12]; and physical function assessed by the FRl. [13] Secondary outcomes were treatment satisfaction (5 response options ranging from very dissatisfied to very satisfied), [18] global perceived change (11–point scale ranging from – 5 to 5), [19] and minimal acceptable outcome (MAO). [20] We also administered at baseline the Pain Catastrophising Scale, [21] STarT Back Screening Tool, [22] and the Fear Avoidance Beliefs Questionnaire. [23] Participants' ability to determine which group they had been allocated to was assessed by the Bang Blinding Index. [17] All outcome measures were assessed at 2–week follow-up.
Statistical Analysis
Our a priori sample size estimation for the primary analysis was based on detecting a 20% difference in the occurrence of adverse events between the 2 treatment groups. This analysis required the recruitment of 180 study participants as necessary to achieve 80% power. In this analysis, we were interested in measuring differences in treatment outcome comprising the minimal clinically important differences (MCIDs) of 9 points on the FRF [24] and 2 points on the NRS. [25] Considering variance estimates from previous studies, [24, 25] and alpha equal to 0.05, we achieved 82% and 99% power to detect clinically important between-group differences in physical function and pain intensity, respectively.
Data were analyzed using SPSS version 21 (IBM Corp., Armonk, NY). Treatment effects were estimated using separate, random-intercept linear mixed models for the outcomes of pain intensity and physical function. Time (baseline and 2–week follow-up) and treatment group (sham or usual chiropractic) were modeled as fixed effects. The hypothesis of interest was the time by group interaction, which we examined with pair-wise comparisons of the estimated marginal means. We included sex and the baseline score of the outcome variable as covariates. Gonsistent with the intention to treat priticiple, the linear mixed models estimated values for missing data based on available scores; therefore all assigned participants were included in the analyses.
Global perceived change was dichotomized by using a cutoff point of 2 or more, leaving 2 categories "improved" and "not improved." We assessed MAO by calculating the proportion in each group who achieved their MAO value. [20] Treatment satisfaction was dichotomized by combining "satisfied" and "very satisfied" and combining "no preference," "dissatisfied," and "very dissatisfied," leaving 2 categories "satisfied" and "not satisfied." The proportions of participants reporting global improvement, achieving a MAO and experiencing treatment satisfaction were compared using logistic regression. Participant sex was modeled as a covariate. Missing data were handled with multiple imputation using Rubin rules. [26]
Finally, we used bivariate logistic regression to examine the relationship between treatment satisfaction and the following clinical and outcome variables: group assignment; age; sex; baseline pain intensity; baseline physical function; Pain Gatastrophising Scale summary scale total, along with rumination, magnification, and helplessness subscale totals; Fear Avoidance Beliefs Questiormaire Work and Physical Activity subscale scores; low, moderate, and high-risk STarT Back subgroups [22]; adverse event oeeurrenee (Yes/No, based on partieipant's subjective assessment); meeting MCID threshold for the NRS and FRI; meeting the MAO; and blinding success.
RESULTS
Study Population

Table 1
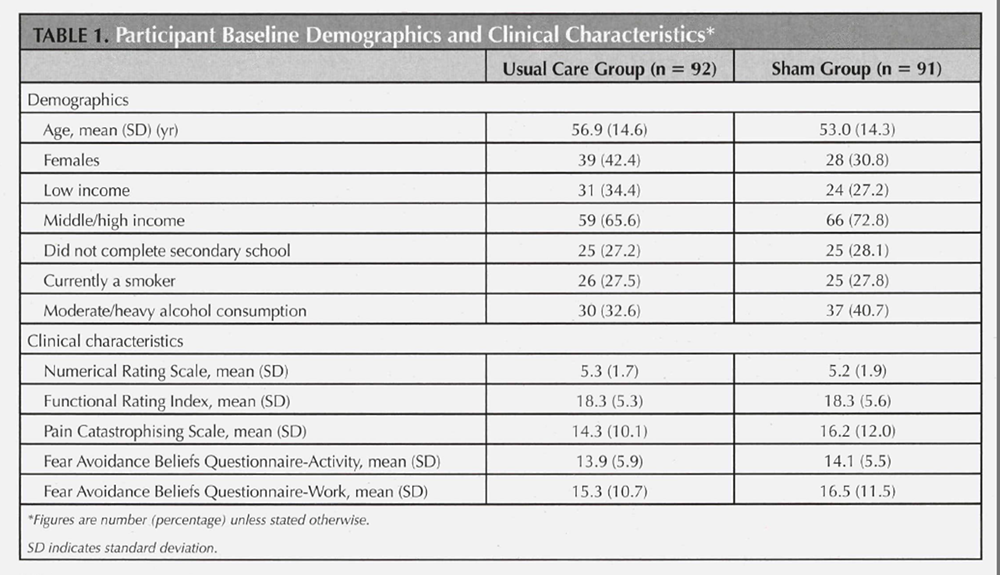
Participants Of the 272 potential participants we screened, 198 satisfied selection criteria. One hundred eighty three participants were randomized to the sham intervention group (n = 91) or usual care group (n = 92). Participant flow through the study is displayed in Figure 1.
There were no important baseline differences in démographie details or clinieal eharacteristics, except for a higher percentage of females in the usual care group (42% compared with 31%). Participant baseline demographic details and clinical characteristics are displayed in Table 1.
At baseline, the overwhelming majority of patients (98%) had experienced spinal pain for more than 3 months. Threequarters had experienced spinal pain for more than 5 years (75% in the sham group; 73% in the usual care group). The vast majority indicated that it had been more than 1 year since last experiencing a 4–week pain-free period (89% in the sham group; 98% in the usual care group), and more than twothirds reported it had been more than 1 year sinee experieneing a pain-free period of at least 1 week (71% in the sham group; 68% in the usual care group).
Chiropractors In total, 8 chiropractors (5 males) provided usual care and 4 chiropractors (2 males) delivered the sham intervention. Chiropractors in the sham group had an average 3.6 (SD, 1.1) years clinical experience whereas chiropractors delivering usual care had an average 12.6 (SD, 2.3) years clinical experience. Most ehiropraetors had obtained their qualifieations from Australian universities (8/11). All ehiropraetors were registered with the national regulatory board and praetieed fulltime.
Type of Therapies Used in Usual Care Group
Table 2
Table 3
Table 4
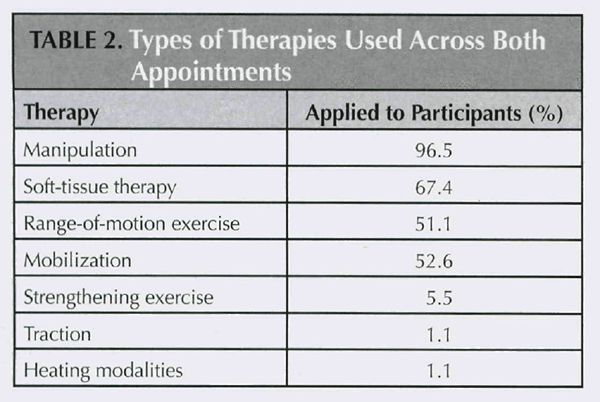
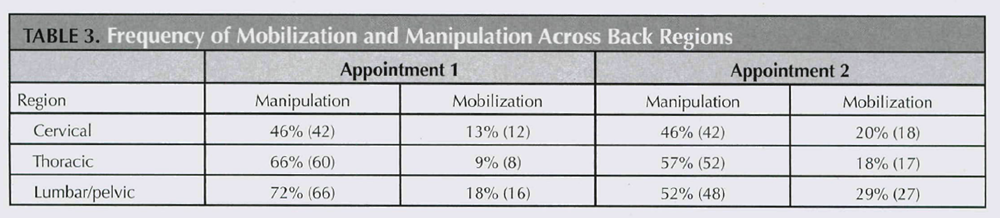
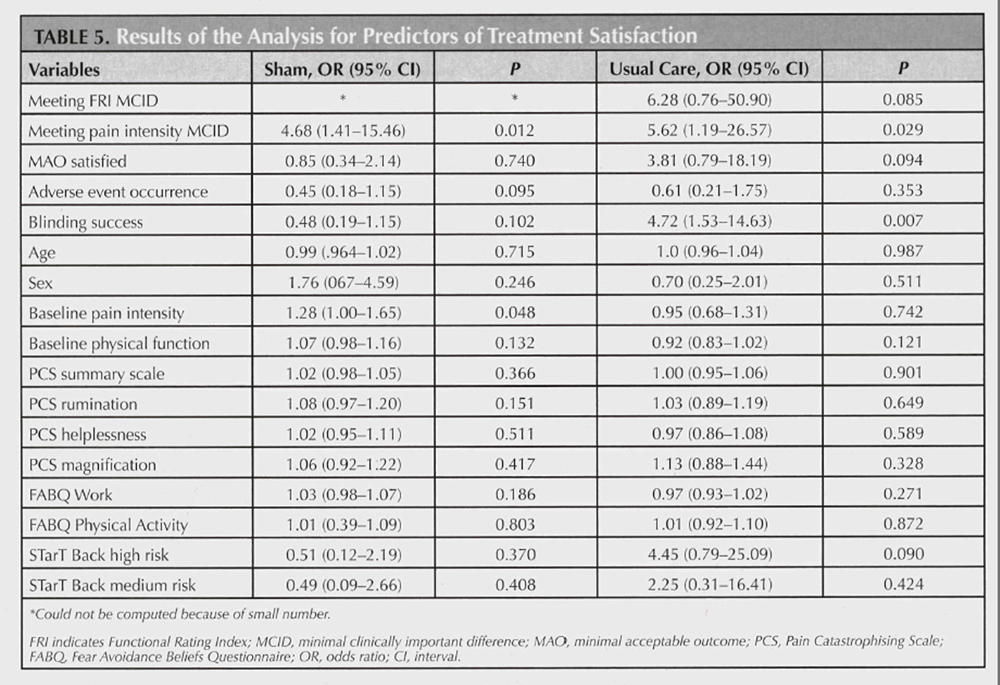
Table 5 Details about the speeifie therapies applied to participants in the usual care group are displayed in Table 2. The frequency of manipulation and mobilization at eaeh spine region are displayed in Table 3.
Outcomes at 2 Weeks
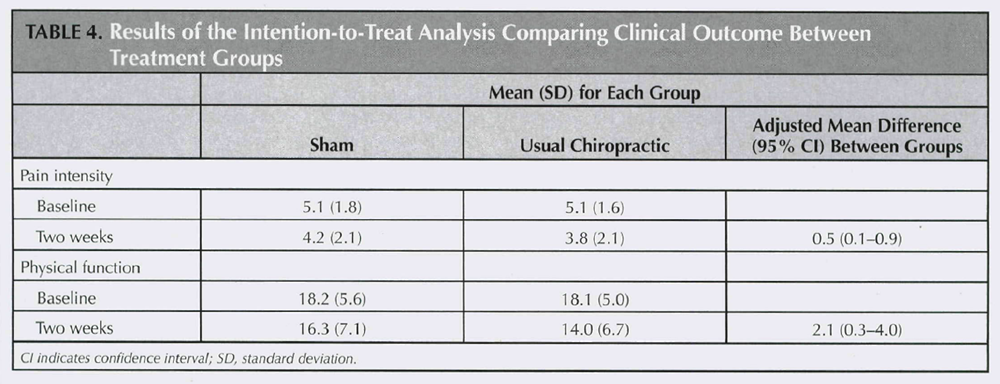
Partieipants reeeiving usual ehiropraetie care experienced greater improvements in pain intensity and physical function than participants reeeiving the sham intervention (Table 4). However, the observed differenees in treatment outcome were not elinieally important. More participants experienced global improvement when receiving the usual chiropractic care than the sham intervention (48% improved vs. 24% improved, ? = 0.012). For MAO, 34% of the sham group, and 29% of the usual care group, partieipants met their speeified threshold. There was no signifieant differenee between groups in the proportion of partieipants who met their MAO (P = 0.42).
Greater treatment satisfaction was reported by those in the usual chiropractic group in comparison to those receiving the sham intervention (78% satisfied vs. 56% satisfied, P = 0.004). For the usual care group, the only significant predictors of treatment satisfaction were meeting the MGID threshold for pain intensity (odds ratio = 5.6:, 95% GI = 1.2–26.6) and correctly identifying group assignment (odds ratio = 4.7; 95% GI = 1.5–14.6) (Table 5). For the sham group, the only significant predictor of treatment success was meeting the MGID threshold for pain intensity (odds ratio = 4.6; 95% GI = 1.5–15.5) (Table 5).
The proportion of participants who correctly identified their assigned treatment was 67% for the sham group and 85% for the usual care group. Bang Index values showed that 25% of the sham group (95% GI = 10%–40%) and 6 1% of the usual care group (95% GI = 48%–74%) guessed correctly beyond what would be expected by chance. [17]
There were no serious adverse events. Gommon adverse events were increased pain (sham group, 29%; usual care group, 36%), muscle stiffness (sham group, 29%; usual care group, 37%), and headache (sham group, 17%; usual care group, 9%).
DISCUSSION
This seems to have been only the second study to use a shamcontrolled design to examine the effectiveness of chiropractic treatment. Our finding that chiropractic treatment for spinal pain produced a statistically significant difference, but not a clinically meaningful difference, is consistent with the results of that previous study. [27] Gonsidering spinal manipulation more broadly, the finding that usual chiropractic treatment is not superior to sham intervention is also consistent with some, [28, 29] but not all, [30–33] previous studies. Hence, this study adds to the body of knowledge exploring whether spinal manipulation for spinal pain provides an advantage compared with sham intervention.
The small treatment effects observed in our study, and indeed others, may result from the chiropractors treating nonspecific spinal pain as a homogenous condition rather than a collection of conditions with differing etiologies. [34] If notispecific spinal pain does consist of heterogeneous conditions, then a specific intervention such as chiropractic treatment may be only effective in select cases. [6, 34] Previous studies have identified a subgroup of patients with low back pain who are likely to achieve clinical success with SMT. [35, 36] The topic of subgrouping patients with nonspecific spinal pain has been subject to much debate. [37–40] If additional studies are conducted it may or may not define the subgroup of patients with spinal pain better suited to chiropractic therapy.
The MAO has been proposed as an alternative method to evaluate clinical outcome, based on a prospective minimum threshold established by each patient. [20] In comparison to the MCID, it provides a different perspective on treatment success because not all patients have the same goal, and it enables an evaluation of how frequently individual patient goals are met. [20] In contrast to the other study outcomes, we found no betweengroup difference in the proportion of participants achieving their MAO. This finding adds to the complexity of identifying the effectiveness of therapies for spinal pain and may highlight the natural fluctuations experienced by patients with spinal pain and the impact of nonspecific treatment effects.
In line with previous studies, we found that treatment satisfaction was related to patients meeting the threshold for MCID. [41, 42] But it was surprising that reaching the MAO threshold was not associated with treatment satisfaction because a previous study had shown it to be a strong predictor of satisfaction. [20] However, that study was the only one to have examined the relationship between MAO and treatment satisfaction, which suggests further studies are required to clarify this relationship. [20]
The strengths of our study included a rigorous concealed randomization procedure, blinded outcome assessors, the use of valid, reliable outcome measures, and providing treatment in a typical chiropractic setting. There were also several limitations. First, we were generally unsuccessful in our attempt to blind study participants to group allocation. This probably resulted from inherent difficulties in identifying a credible sham intervention for use in a chiropractic trial, or indeed many types of randomized controlled trial. [43] Also, we did not ask the participants if they had previously received chiropractic treatment. If the sham group contained a reasonable number of nonnaive participants, then this may have impacted substantially on the success of the blinding procedure. Nonetheless, short of using more aggressive blinding procedures such as conscious sedation, it may not be possible to blind participants successfully in trials involving treatments such as manual therapy and exercise. [44]
Second, offering only 2 treatments may not reflect typical chiropractic practice and recommendations from clinical guidelines. [45–47] However, other studies of chiropractic effectiveness have only provided 2 treatments and the evidence suggests that outcomes after 2 chiropractic visits are predictive of subsequent improvement. [6, 9, 48, 48]
Third, we did not assess either anxiety or depression, and differing levels of anxiety or depression may potentially have affected clinical outcomes in either group. However, no important differences were observed between groups in the psychosocial characteristics measured at baseline including the Pain Catastrophising Scale and Fear Avoidance Beliefs Questionnaire. Finally, the chiropractors delivering the sham intervention were less experienced than the chiropractors providing usual care. However, clinician experience does not seem to infiucncc clinical outcome among patients receiving spinal manipulative therapy, [50] and in any event the chiropractors delivering sham did not provide spinal manipulative therapy.
CONCLUSION
Future research should concentrate on identifying clinically relevant spinal pain subgroups to which chiropractic and other manual therapy treatments may be best suited. It would also be worthwhile to identify credible sham interventions and to conduct studies examining how nonspecific effects, such as interpersonal attributes, contribute to treatment outcomes.
Key Points
Participants receiving chiropractic therapy reported greater improvements in pain and physical function.
Chiropractic therapy for spinal pain did not produce a clinically important effect.
Awareness of treatment assignment and achieving minimally important improvement in pain intensity were associated with chiropractic therapy satisfaction.
References:
Lim SS, Vos T, Flaxman AD, et al.
A comparative risk assessment of burden of disease and injury attriburable to 67 risk factors
and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010.
Lancet 2012;380:2224-60.Dagenais S, Caro J, Haldeman S.
A Systematic Review of Low Back Pain Cost of Illness Studies
in the United States and Internationally
Spine J 2008 (Jan); 8 (1): 8–20Walker BF, Müller R, Grant WD.
Low back pain in Australian adults. Health provider utilization and care seeking.
J Manipulative Physiol Ther 2004;27:327-35.Cote P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, et al.
The Burden and Determinants of Neck Pain in Workers: Results of the Bone and Joint Decade
2000–2010 Task Force on Neck Pain and Its Associated Disorders
Spine (Phila Pa 1976). 2008 (Feb 15); 33 (4 Suppl): S60-74Lambeek LC, van Tulder MW, Swinkels IC, et al.
The trend in total cost of back pain in the Netherlands in the period 2002 to 2007.
Spine 2011;36:1050-8.Walker BF, French SD, Grant W, et al.
Combined chiropractic interventions for low-back pain.
Cochrane Database Syst Rev 2010;4:CD005427.Gross A, Miller J, D’Sylva J, Burnie SJ, Goldsmith CH, Graham N, et al.
Manipulation or Mobilisation For Neck Pain: A Cochrane Review
Manual Therapy 2010 (Aug); 15 (4): 315–333Rubinstein SM, Terwee CB, Assendelft WJ, et al.
Spinal manipulative therapy for acute low back pain: an update of the Cochrane review.
Spine (Phila Pa 1976) 2013;38:E158-77.Rubinstein SM, van Middelkoop M, Assendelft WJ, et al.
Spinal manipulative therapy for chronic low-back pain: an update of a Cochrane review.
Spine (Phila Pa 1976) 2011;36:E825^6.Walker, BF, Hebert, JJ, Stomski, NJ et al.
Outcomes of Usual Chiropractic.
The OUCH Randomized Controlled Trial of Adverse Events
Spine (Phila Pa 1976). 2013 (Sep 15); 38 (20): 1723–1729Walker B, Losco B, Clarke B, et al.
Outcomes of usual chiropractic, harm & efficacy, the ouch study: study protocol for a randomized controlled trial.
Trials 2011;12:235.Katz J, Melzack R.
Measurement of pain.
Surg Clin North Am 2010;79:231-52.Feise RJ, Michael Menke J.
Functional rating index: a new valid and reliable instrument to measure the magnitude of clinical change
in spinal conditions.
Spine (Phila Pa 1976) 2001;26:78-86; discussion 87.Costa LO, Maher CG, Latimer J, et al.
Motor control exercise for chronic low back pain: a randomized placebo-controlled trial.
Phys Ther 2009;89:1275-86.Gemmell H, Miller P.
Comparative effectiveness of manipulation, mobilisation and the activator instrument in treatment
of non-specific neck pain: a systematic review.
Chiropr Osteopat 2006;14:7.Australian Musculoskeletal Pain Guidelines Group.
Fvidence-based management of acute musculoskeletal pain.
Nati Lihr Aust 2003 2003:1-80.Bang N, Ni L, Davis C.
Assessment of blinding in clinical trials.
Control Clin Trials 2004;25:143-56.Dworkin RH, Turk DC, Wyrwich KW, et al.
Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations.
J Pain 2008;9:105-21.Kamper S, Maher C, Mackay G.
Global rating of change scales: a review of strengths and weaknesses and considerations for design.
J Man Manip Ther 2009;17:163-170.Carragee E, Cheng 1.
Minimum acceptable outcome after lumbar spinal fusion.
Spine J 2010;10:313-20.Sullivan M, Bishop S, Pivik J.
The pain catastrophizing scale: development and validation.
Psychol Assess 1995;7:524-32.Hill JC, Dunn KM, Lewis M, et al.
A primary care back pain screening tool: identifying patient subgroups for initial treatment.
Arthritis Rheum 2008;59:632-4LWaddell G, Newton M, Henderson I, et al.
A Fear-Avoidance Beliefs Questionnaire (FABQ) and the Role of Fear-avoidance Beliefs
in Chronic Low Back Pain and Disability
Pain. 1993 (Feb); 52 (2): 157–168Childs JD, Piva SR.
Psychometric properties of the functional rating index in patients with low back pain.
Eur Spine J 2005;14:1008-12.Childs J, Piva SR, Fritz JM.
Responsiveness of the Numeric Pain Rating Scale in patients with low back pain.
Spine 2005;30:1331-4.Rubin DB.
Multiple Imputation for Nonresponse in Surveys.
New York: John Wiley &Sons;í997.Waagen GH, Haldeman S, Cook G, et al.
Short term trial of chiropractic for the relief of chronic low back pain.
Manu Med 1986;2:63-7.Ghroubi S, Elleuch H, Baklouti S, et al.
Chronic low back pain and vertebral manipulation.
Ann Readapt Med Phys 2007;50:570-76.Licciardone JC, Stoll ST, Fulda KG, et al.
Osteopathie manipulative treatment for chronic low back pain: a randomized controlled trial.
Spine (Phila Pa 1976) 2003;28:1355-62.Cleland JA, Childs JD, McRae M, et al.
Immediate effects of thoracic manipulation in patients with neck pain: a randomized clinical trial.
Man Ther 2005;10:127-35.Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, et al.
Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial.
J Orthop Sports Phys Ther 2009;39:20-7.Vernon HT, Aker P, Burns S, et al.
Pressure pain threshold evaluation of the effect of spinal manipulation in the treatment of
chronic neck pain: a pilot study.
J Manipulative Physiol Ther 1990;13: 13-6.Licciardone JC, Minotti DE, Gatchel RJ, et al.
Osteopathie manual treatment and ultrasound therapy for chronic low back pain:
a randomized controlled trial.
Ann Fam Med 2013;l 1:122-9.Hebert JJ, Koppenhaver SL, Walker BE
Subgrouping patients with low back pain: a treatment-based approach to classification.
Sports Health 20n-3:534-A2.Childs JD, Fritz JM, Flynn TW, Irrgang JJ, Johnson KK, Majkowski GR, et al.
A Clinical Prediction Rule To Identify Patients With Low Back Pain Most Likely To Benefit
from Spinal Manipulation: A Validation Study
Annals of Internal Medicine 2004 (Dec 21); 141 (12): 920–928Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D. et al.
A Clinical Prediction Rule for Classifying Patients with Low Back Pain
who Demonstrate Short-term Improvement with Spinal Manipulation
Spine (Phila Pa 1976). 2002 (Dec 15); 27 (24): 2835–2843Fitzgerald GK.
Invited commentary.
Phys Ther 2010;90:855-8; author reply 858.Hancock M, Herbert RD, Maher CG.
A guide to interpretation of studies investigating subgroups of responders to physical therapy interventions.
Phys Ther 2009;89:698-704.Hebert JJ, Fritz JM.
Clinical decision rules, spinal pain classification and prediction of treatment outcome:
a discussion of recent reports in the rehabilitation literature.
Chiropr Man Therap 2012; 20:19.Stanton TR, Hancock MJ, Maher CG, et al.
Critical appraisal of clinical prediction rules that aim to optimize treatment selection for musculoskeletal conditions.
Phys Ther 2010;90:843-54.Dworkin RH, Jensen MP, Gould E, et al.
Treatment satisfaction in osteoarthritis and chronic low back pain: the role of pain, physical and
emotional functioning, sleep, and adverse events.
J Pain 2011;12:416-24.Jensen MP, Martin SA, Cheung R.
The meaning of pain relief in a clinical trial.
J Pain 2005;6:400-6.Boutron I, Estellat C, Guittet E, et al.
Methods of blinding in reports of randomized controlled trials assessing pharmacologie treatments:
a systematic review.
PLoS Medicine 2006;3:e425.Kawchuk GN, Haugen R, Fritz J.
A True Blind for Subjects Who Receive Spinal Manipulation Therapy
Arch Phys Med Rehabil 2009 (Feb); 90 (2): 366–368National Institute for Health and Clinical Excellence (NICE).
Low Back Pain: Early Management of Persistent Nonspecific Low Back Pain
London: National Institute for Health and Care Excellence; 2009.
[Report No.: Clinical guideline 88].Airaksinen O, Brox JI, Cedraschi C, et al.
COST B13 Working Group on Guidelines for Chronic Low Back Pain Chapter 4.
European Guidelines for the Management of Chronic Nonspecific Low Back Pain
European Spine Journal 2006 (Mar); 15 Suppl 2: S192–300Chou R, Huffman LH; American Pain Society.
Nonpharmacologic Therapies for Acute and Chronic Low Back Pain:
A Review of the Evidence for an American Pain Society/
American College of Physicians Clinical Practice Guideline
Annals of Internal Medicine 2007 (Oct 2); 147 (7): 492–504Gross A, Miller J, D'Sylva J, et al.
Manipulation or mobilisation for neck pain.
Cochrane Database Syst Rev 2010;20:CD004249.Ghilds JD, Fritz JM, Piva SR, et al.
Proposal of a classification system for patients with neck pain.
J Orthop Sports Phys Ther 2004;34:686-96; discussion 697-700.Whitman JM, Fritz JM, Childs JD.
The influence of experience and specialty certifications on clinical outcomes for patients with low back pain
treated within a standardized physical therapy management program.
J Orthop Sports Phys Ther 2004;34:662-72; discussion 672—5.

Return to SPINAL PAIN MANAGEMENT
Since 2-20-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |