

The Biomechanics of Spinal Manipulation This section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: J Bodyw Mov Ther. 2010 (Jul); 14 (3): 280–286 ~ FULL TEXT
Walter Herzog, PhD
Faculty of Kinesiology,
University of Calgary,
Calgary, AB T2N 1N4, Canada.
walter@kin.ucalgary.caBiomechanics is the science that deals with the external and internal forces acting on biological systems and the effects produced by these forces. Here, we describe the forces exerted by chiropractors on patients during high-speed, low-amplitude manipulations of the spine and the physiological responses produced by the treatments. The external forces were found to vary greatly among clinicians and locations of treatment on the spine. Spinal manipulative treatments produced reflex responses far from the treatment site, caused movements of vertebral bodies in the "para-physiological" zone, and were associated with cavitation of facet joints. Stresses and strains on the vertebral artery during chiropractic spinal manipulation of the neck were always much smaller than those produced during passive range of motion testing and diagnostic procedures.
Keywords: Spinal manipulation; Mobilization; Continuous passive motion; Manipulable lesion; Functional spinal lesion; Subluxation; Biomechanics

From the FULL TEXT Article:
Introduction
Chiropractic spinal manipulations are mechanical events. Clinicians exert a force of specific magnitudein a controlled direction to a target site,typically on the spine. High-velocity, low-amplitude (HVLA) manipulations are more frequently used by chiropractors than other treatment modalities, and they are of special interest, as force magnitudes and the rates of force application are high. HVLA treatments cause deformations of the spine and surrounding soft tissues and often elicit a cracking sound that has been identified as cavitation of spinal facet joints (Cascioli et al.,2003; Conway et al.,1993; Haas,1990; Herzog et al., 1993c; Mealand Scott, 1986; Miereau et al., 1988; Reggars,1996). Despite the acknowledged nature of mechanical force application as a treatment modality (Triano,2000), and the accepted idea that HVLA treat ments produce mechanical effects (e.g., Triano and Schultz, 1997) at the treatment site, little is known about the biomechanics of spinal manipulation.
Biomechanics is the science that deals with the external and internal forces acting on biological systems and the associated effects produced by these forces. Here, I will attempt to briefly review what is known about the external forces applied by chiropractors during HVLA manipulative treatments on patients, discuss selected effects of these forces, and then focus specifically on an increasingly important topic of internal force transmission: the stresses and strains experienced by the vertebral artery during HVLA neck manipulations.
External forces applied by chiropractors during HVLA spinal manipulations
Wood and Adams (1984) and Adams and Wood (1984) were the first to quantify the forces exerted by chiropractors during spinal manipulation. Their work involved application of a HVLA manipulative thrust to a treatment dummy. Although a classic piece, the limitation of their work was that treatments were not performed on human subjects, thereby bringing into question the validity of the results for a clinical setting. Hessel et al. (1990) were the first to directly measure the forces applied by chiropractors on human subjects for a variety of different treatment modalities. They used a thin, flexible pressure pad that was placed under the thrusting hand of the clinician to measure the forces applied to the target site on patients. This pioneering work was followed by a series of similar studies, all aimed at obtaining information on the orce-time histories of HVLA spinal manipulations (Conway etal., 1993; Herzog et al., 1993 a,b; Kawchuk et al., 1992; Kawchuk and Herzog, 1993; Triano and Schultz, 1997; Triano, 2000; Triano and Schultz,1990).
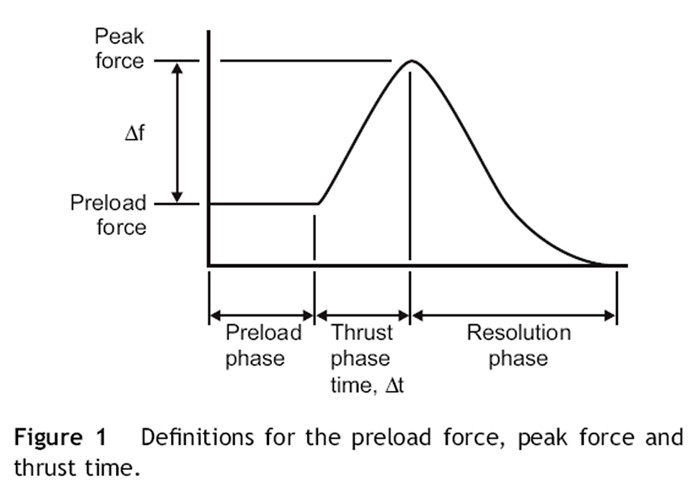
Figure 1

Table 1

Figure 2

Figure 3 When combining the results of selected force parameters during HSLA treatments,the following results emerged: Peak and Preload forces (Figure 1) varied dramatically depending on the location of treatment application (Herzog et al., 1993a). Peak forces for neck manipulations (on average about 100N) were substantially smaller than the peak forces applied during thoracic and lumbar spine and sacroiliac joint treatments (allabout 400N (Table1)). Furthermore,the treatment forces varied dramatically between clinicians, and in our laboratory we have measured peak forces ranging from 200N to 1600N (Herzog et al.,1993a), which is an eight- fold difference. Figure 2 shows a random sample of ten female and ten male chiropractors performing treatments on a small number of subjects (Forand et al., 2004). Interestingly, the average forces between males and females are about the same (Forand et al., 2004) (Figure 3)), and so are the average forces between novice and experienced chiropractors (results not shown).
From these direct measurements of the external forces applied by clinicians on patients,the following conclusions seem warranted:
The external forces applied during HVLA treatments vary dramatically depending on the treatment site
The external forces applied during HVLA treatments vary dramatically across clinicians.
These results suggest that local mechanical conditions might affect the amount of force applied by clinicians. For example, all clinicians apply substantially less force for treatments of the cervical spine compared to the thoracic spine (Herzog et al.,1993a). The reasons for this observation are not clear, although it makes intuitive sense that a relatively mobile part of the spine (cervical spine) would be treated differently than a relatively stiff segment of the spine (thoracic spine). The amount of force applied to patients by a given chiropractor varies dramatically as indicated above (Conway et al.,1993; Herzog,1991; Herzog et al.,1993a,b; Kawchuk et al.,1992; Triano,2000). Clinicians, who tend to adjust with great force, do so consistently and clinicians who use little force do so consistently as well.
Some “soft” adjusting clinicians will not even reach the preload forces of some of the “hard” adjusting clinicians, thus it is questionable whether force magnitude is an important variable in the application of a HVLA chiropractic treatment. The thrust times (Figure 1) were approximately 100ms for cervical and 150ms for thoracic and lumbar spine treatments. Since the peak force magnitudes vary substantially and thrust times are similar across practitioners, it follows that the rate of force application varies substantially too (Table1), and thus is likely not a relevant factor for the success of a chiropractic treatment. In the absence of consistent force-time histories for chiropractic manipulations, one may conclude that the detailed force magnitude might not be an important characteristic for the success of a treatment, while the thrust direction might be. Unfortunately, thrust force directions have not been studied systematically, thus this proposition must be considered a hypothesis at present.
Selected effects of HVLA spinal manipulative treatments
There are many scientific and clinical publications advertising the efficacy of HVLA spinal manipulation. However, the number of publications investigating mechanical, physiological or neurological effects produced by such treatments is small, and a direct link between the treatment forces, the effects produced by these forces, and the beneficial effects created are almost completely missing. Here, I would like to discuss just some selected effects of HSLA treatments that have been debated intensely.
Relative movements of the target segment in the paraphysiological zone
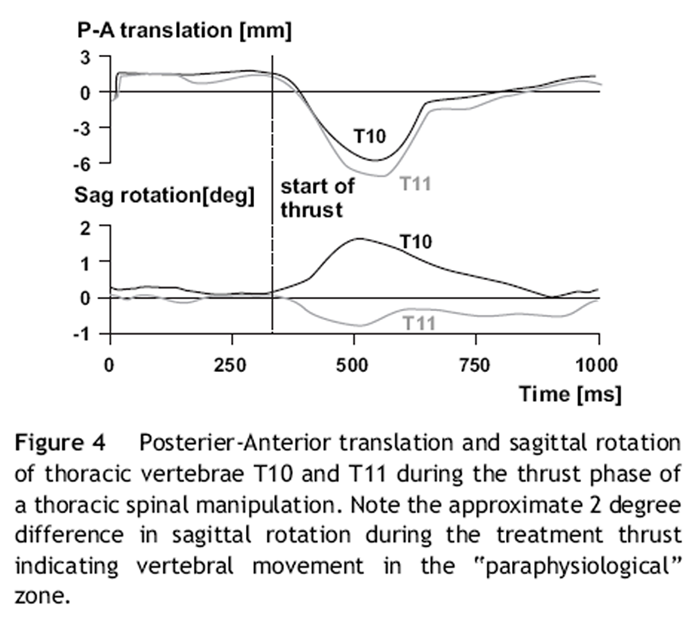
Figure 4 One of the premises of HVLA spinal manipulative treatments has been that the target joint (typically a spinal facet joint) is brought to its end range of motion by the application of a directed and well described preload force ((Triano,2000) (Figure 1)). Following application of the preload force, a force thrust is given that represents the actual treatment, and the idea has been that this thrust force takes the (facet) joint beyond its regular end range of motion into the paraphysiological movement zone. Of course, when applying a thrust, every clinician can feel the deformation of the spine under the thrusting hand, however, it was not possible to decide if part of this movement arose from the target joint, or if the entire deformation was caused by joints neighbouring the target joint that were not brought to the endrange of motion by preload force application. In order to study this question in detail, we inserted bone pins into three adjacent vertebral bodies of the thoracic spine in human cadavers, and then calculated the relative movements of the vertebral bodies during the preload and the thrust phase of HVLA anterior to posterior thrusts to the transverse process of a thoracic vertebra (Gal et al.,1994,1997a,b). There was substantial relative movement of the target and adjacent vertebrae during the preload phase, and there was further relative movement of target and adjacent vertebrae during the thrust phase of the manipulative treatment (Figure 4). This result illustrates that there is movement of the target (facet) joint during thrust application beyond the movement achieved by the preload force (Gal et al.,1994, 1997a,b).
Reflex responses associated with HVLA spinal manipulative treatments

Figure 5
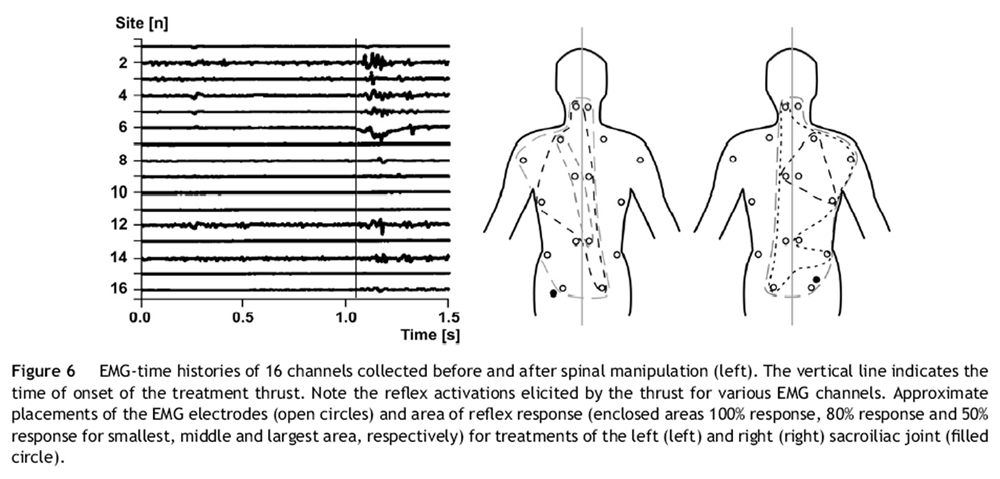
Figure 6
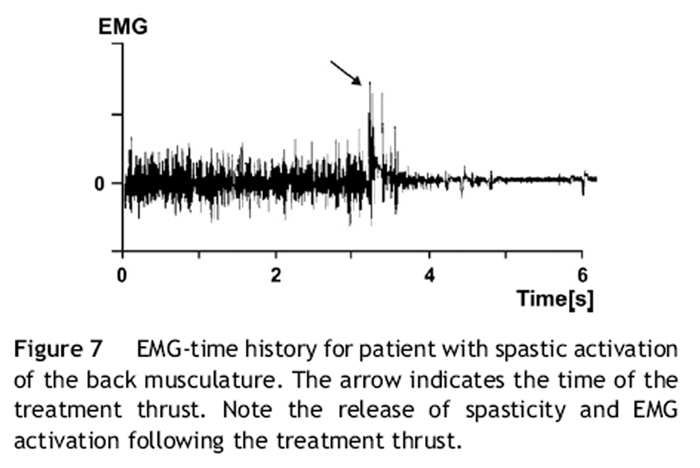
Figure 7 Spinal manipulative treatments, although aimed primarily at restoring joint (including facetjoint) mobility and function, had been thought to produce reflex responses in the muscles underlying the treatment area. In order to test this hypothesis, we measured the surface electromyogram (EMG)of back muscles at the treatment site. Typically, EMG activity was measured within 200-400 ms following the onset of the treatment thrust (Herzog et al.,1995). Muscle activity disappeared following the treatment thrust, and was not observed during preload application, suggesting that this was indeed a reflex response, and that the reflex response was associated with the speed of force application (Figure 5).
When applying a very short and precisely focused treatment force (using an activator instrument), a reflex response was elicited that had the visual shape of a single motor unit action potential. Furthermore,its delay from the onset of force application (50-100 ms) was such that it was suggested to be a muscle spindle reflex pathway (Herzog et al.,1995). Reflex responses produced by activator application were always restricted to the vicinity of treatment application. For HVLA spinal manipulations,the reflex responses were not restricted to the immediate treatment area, but formed characteristic activation patterns that depended on the site of force application ((Herzog et al.,1995,1999) (Figure 6)). Finally, patients presenting with spastic muscles showed EMG activity in the muscles of the treatment area. When subjected to a HVLA treatment thrust, the muscles relaxed and EMG activity was abolished in some but not all of the patients (Herzog, 2000) (Figure 7). It is not known why treatments produced a relief of muscle spasticity in some patients but not in others. We conclude from these observations that HVLA spinal manipulative treatments elicit a reflex response that is not necessarily localized, and affects locations that are remote from the actual treatment site.
Role of the audible release
The audible release, or cracking sound, is an indicator of a successful treatment for many chiropractors, so much so, that when an audible release does not occur, many clinicians will immediately apply a second or even third treatment thrust. The role of the audible release has been a matter of intense debate (Brodeur,1995; Sandoz, 1969) and one of the roles associated with the audible release has been the idea that it causes the reflex responses discussed above. However,there are a variety of observations that do not fit that idea. For example, every HVLA treatment thrust we have recorded was associated with an electromyographical response, but not all of these caused cavitation (Conway et al., 1993). That is, reflex responses were observed in the absence of cavitation. However, in order to address this question directly, we asked chiropractors to apply treatment forces at the exact location and exact direction as they would for a normal manipulative thrust, but to do so very slowly. With a slow force application, an audible release can be elicited, but this release is not associated with a corresponding EMG response (Conway et al., 1987), suggesting that the audible release is not responsible for the observed reflex responses during HVLA chiropractic spinal manipulations.
Internal stresses and strains during HSLA manipulative treatments of the cervical spine
One major issue with the use of HVLA spinal manipulation is its safety, especially with respect to neck manipulation and the risk of stroke. Estimates of the risk of stroke vary from 1:5000 to 1:10 million (Cote et al.,1996; Frisoni and Anzola, 1991; Haldeman et al., 1999, 2002; Hurwitz et al., 1996; Lee et al., 1995). Although the proposed risk is extremely small, the serious and irreversible nature of vascular accidents makes this an important issue (Terrett and Kleynhans, 1980). The earliest documented reports of fatal vascular accidents following spinal manipulation can be traced back to the 1930s (Foster vs Thornton, 1934), and 1940s (Pratt-Thomas and Beyer, 1947). The majority of these cases have involved the vertebrobasilar system, specifically the cephalad/distal loop of the vertebral artery, as it exits the foramen transversarium of C1 (Haldeman etal., 1999). Because of the unique configuration of the vertebral artery, it has been suggested that it experiences considerable stretch and associated tissue stress during extension and rotation of the neck which may lead to occlusion and damage to the arterial walls (Terrett and Kleynhans, 1980). Consequently, it has been hypothesized that HVLA spinal manipulation may also lead to stretch-induced vertebral artery damage, although our biomechanical evidence does not support this view (Herzog and Symons, 2002; Symons et al., 2002).
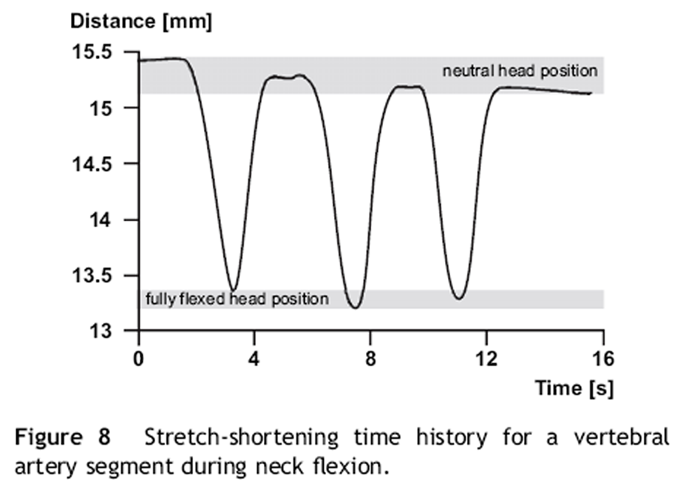
Figure 8
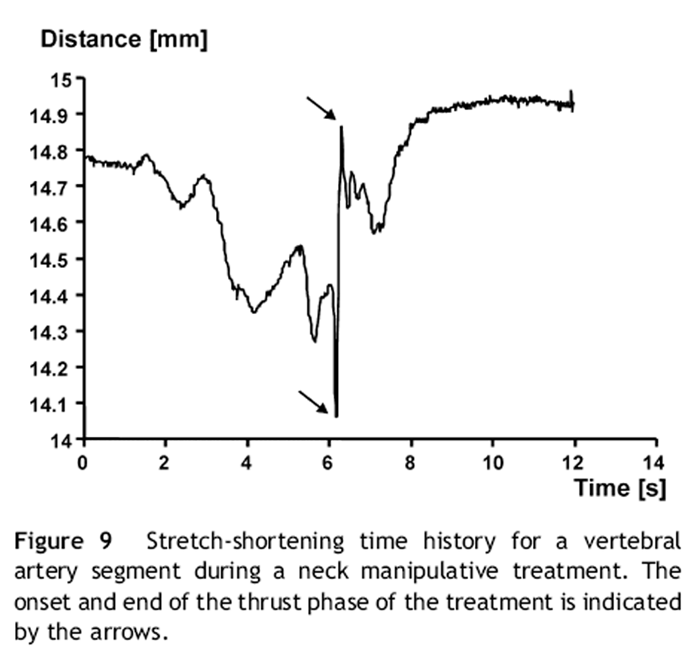
Figure 9

Figure 10 Measurements of internal stresses of soft tissues caused by spinal manipulation are rare, and the only documented reports of such measurements on the vertebral artery are thoseby Herzog and Symons (2002), and Symons et al. (2002). In these studies, the strains of the vertebral artery were measured from the neutral length (head and neck in the neutral position) for a variety of range of motion and diagnostic testing, as well as for different HVLA cervical spine manipulations across all levels performed ipsi- and contralaterally to the target vertebral artery (Figures 8 and 9). They then excised the vertebral arteries carefully from the cadaveric specimens used for these studies and measured the corresponding forces experienced by the vertebral arteries for the strains (elongations) measured during the diagnostic and clinical procedures.
Symons et al. (2002) and Herzog and Symons (2002) found that stretches to the vertebral artery during neck manipulative procedures (6% for the cephalad/distal segment) were much smaller than the stretches produced during range of motion and diagnostic testing (13%). They also found that the elongations produced during HVLA spinal manipulations did not produce any tensile forces in the vertebral artery, suggesting that the vertebral arteries were slack when the head and neck were in the neutral position and that this slack was not fully taken up during spinal manipulative treatments. Therefore, spinal manipulation did not cause any tensile stress in the vertebral arteries during the treatment procedures.
However, the studies by Symons et al. (2002) and Herzog and Symons (2002) had several limitations. Most importantly, measurements were only made for two segments (cephalad to C1 and caudad to C6), forces during the spinal manipulations were not measured and the vertebral arteries of the unembalmed cadavers were devoid of fluid, thus possibly affecting their shape. In order to overcome these limitations, we performed a pilot study to measure the strains in the vertebral artery segments C1-C6 with the arteries filled with gel and while measuring the forces applied by two chiropractors during all diagnostic and treatment procedures. The forces applied by the chiropractors during spinal manipulations were similar to those administered to patients, thus we may assume that the external mechanics were similar (Figure 10). The peak strain (elongation form neutral) that was measured for any of the 176 treatments procedures was 2.1% while strains for diagnostic procedures were in excess of 10% (flexion 10.1%, rotation 13.0% and Houle’s test 9.4%), suggesting, in agreement with our previous studies, that strains during HVLA cervical spinal manipulations were much smaller than those produced during diagnostic procedures.

Figure 11

Figure 12 In contrast to our previous work, however, the strains measured in adjacent vertebral artery segments were not always intuitively apparent. For example, we found the repeatable (across multiple measurements and across clinicians) result that for some diagnostic and treatment procedures, one vertebral artery segment shortened while the adjacent segment was stretched. Forexample, in Figure 11, we show the right vertebral artery segments C2/C3 and C3/C4 for a left rotation of the neck. Textbook anatomical considerations would suggest that the vertebral artery segments should be stretched, which was observed for the C2/C3 segment, but not the C3/C4 segment which shortened consistently for both chiropractors and for all three repeat measurements. Similarly, these same segments behaved opposite during a HVLA neck manipulation (Figure 12). Again, this result was observed for all three repeat measurements of and both clinicians. Combined, the results of this study suggest that spinal manipulative treatments produce stretches of the vertebral artery that are much smaller than those that are produced during normal everyday movements, and thus they appear harmless. However, textbook anatomical considerations do not necessarily allow prediction of the direction of strain in different vertebral artery segments. Some non-intuitive behaviour was observed that cannot be explained at present but might be related to the intricate coupled motions of vertebral bodies and the complex fixation of the vertebral artery to the transverse foramen of C1-C6.
In summary, there is little knowledge of the transmission of stresses and strains across hard and soft tissues during spinal manipulation. This is a vast field of investigation that needs careful attention so that the detailed mechanics of HVLA treatments can be understood and possible risks of these procedures may be identified.
Acknowledgements
The Canadian Chiropractic Research Foundation, Canadian Chiropractic Protective Association,
The Alberta College and Association of Chiropractors.
References:
Adams, A.H., Wood,J., (1984).
Comparison of forces used in selected adjustments of the lowback: A preliminary study.
Res. Forum 1, 5-9.Brodeur, R., (1995).
The audible release associated with joint manipulation.
Journal of Manipulative and Physiological Therapeutics 18, 155-164.Cascioli, V., Corr, P., TillAg, A.G., (2003).
An investigation in to the production of intra-articular gas bubbles and increase in joint space in the zygapophyseal joints of the cervical spine in asymptomatic subjects after spinal manipulation.
Journal of Manipulative and Physiological Therapeutics 26(6), 356-364.Conway, B.A., Hultborn, H., Kiehn, O., (1987).
Proprioceptive input resets central locomotor rhythm in the spinal cat.
Exp.Brain Res. 68 (3), 643-656.Conway, P.J.W., Herzog, W., Zhang, Y., Hasler, E.M., Ladly, K., (1993).
Forces required to cause cavitation during spinal manipulation of the thoracic spine.
Clinical Biomechanics 8, 210-214.Cote, P., Kreitz, B.G., Cassidy, J.D., Thiel, H., (1996).
The Validity of the Extension-rotation Test as a Clinical Screening Procedure
Before Neck Manipulation: A Secondary Analysis
J Manipulative Physiol Ther 1996 (Mar); 19 (3): 159–164Forand, D., Drover, J., Suleman, Z., Symons, B., Herzog, W., (2004).
The forces applied by female and male chiropractors during thoracic spinal manipulation.
Journal of Manipulative and Physiological Therapeutics 27, 49-56.Foster vs Thornton, (1934).
Medicolegal abstract.
Malpractice: death resulting from chiropractic treatment for headache.
Journal of American Medical Association 103, 1260.Frisoni, G.B., Anzola, G.P., (1991).
Vertebrobasilar ischemia after neck motion.
Stroke 22 (11), 1452-1460.Gal, J., Herzog, W., Kawchuk, G., Conway, P.J.W., Zhang,Y., (1997a).
Movements of Vertebrae during manipulative thrusts to unembalmed human cadavers.
Journal of Manipulative and Physiological Therapeutics 20, 30-40.Gal, J., Herzog, W., Kawchuk, G., Conway, P.J.W., Zhang, Y.T., (1994).
Biomechanical studies of spinal manipulative therapy (SMT): Quantifying the movements of vertebral bodies during SMT.
The Journal of the CCA 38, 11-24.Gal, J., Herzog, W., Kawchuk, G., Conway, P.J.W., Zhang, Y.T., (1997b).
Measurements of vertebral translations using bone pins, surface markers and accelerometers.
Clinical Biomechanics 12 (5), 337-340.Haas, M., (1990).
The physics of spinal manipulation. PartIV. A theoretical consideration of the physician impact force and energy requirements needed to produce synovial joint cavitation.
Journal of Manipulative and Physiological Therapeutics 13, 378-383.Haldeman S, Kohlbeck FJ, McGregor M. (2002).
Unpredictability of Cerebrovascular Ischemia Associated with Cervical Spine Manipulation
Therapy: A Review of Sixty-four Cases After Cervical Spine Manipulation
Spine (Phila Pa 1976) 2002 (Jan 1); 27 (1): 49–55Haldeman, S., Kohlbeck, F.J., McGregor, M., (1999).
Risk Factors and Precipitating Neck Movements Causing Vertebrobasilar Artery Dissection
After Cervical Trauma and Spinal Manipulation
Spine (Phila Pa 1976) 1999 (Apr 15); 24 (8): 785–794Herzog, W. (2000).
Clinical Biomechanics of Spinal Manipulation
Churchill Livingstone, Philadelphia.Herzog, W., Conway, P.J.W., Kawchuk, G.N., Zhang, Y., Hasler, E. M., (1993a).
Forces exerted during spinal manipulative therapy.
Spine 18, 1206-1212.Herzog, W.,Conway, P.J.W., Zhang, Y.T., Gal, J., Guimaraes, A.C. S., (1995).
Reflex responses associated with manipulative treatments on the thoracic spine.
Journal of Manipulative and Physiological Therapeutics 18, 233-236.Herzog, W., Kawchuk, G.N., Conway, P.J.W., (1993b).
Relationship between preload and peak forces during spinal manipulative treatments.
Journal of the Neuromusculoskeletal System 1(2), 52-58.Herzog, W., Scheele, D., Conway, P.J.W., (1999).
Electromyographic responses of back and limb muscles associated with spinal manipulative therapy.
Spine 24 (2), 146-152.Herzog, W., Symons, B., (2002).
The Mechanics of Neck Manipulation With Special Consideration of the Vertebral Artery
J Can Chiropr Assoc. 2002 (Sep); 46 (3): 134–136Herzog, W., Zhang, Y.T., Conway, P.J.W., Kawchuk, G.N., (1993c).
Cavitation sounds during spinal manipulative treatments.
Journal of Manipulative and Physiological Therapeutics 16, 523-526.Hessel, B.W., Herzog, W., Conway, P.J.W., McEwen, M.C., (1990).
Experimental measurement of the force exerted during spinal manipulation using the Thompson technique.
Journal of Manipulative and Physiological Therapeutics 13, 448-453.Hurwitz EL, Aker PO, Adams AH, Meeker WC, Shekelle PG. (1996).
Manipulation and Mobilization of the Cervical Spine:
A Systematic Review of the Literature
Spine (Phila Pa 1976) 1996 (Aug 1); 21 (15): 1746–1760Kawchuk, G.N., Herzog, W., (1993).
Biomechanical characterization (fingerprinting) of five novel methods of cervical spinal manipulation.
Journal of Manipulative and Physiological Therapeutics 16 (9), 573-577.Kawchuk, G.N.,Herzog, W., Hasler, E.M., (1992).
Forces generated during spinal manipulative therapy of the cervical spine: A pilot study.
Journal of Manipulative and Physiological Therapeutics 15, 275-278.Lee, K.P., Carlini, W.G., McCormick, G.F., Albers, G.W., (1995).
Neurologic complications following chiropractic manipulation: a survey of California neurologists.
Neurology 45(6), 1213-1215.Meal, G.M., Scott, R.A., (1986).
Analysis of the joint crack by simultaneous recording of sound and tension.
Journal of Manipulative and Physiological Therapeutics 9(3), 189-195.Miereau, D., Cassidy, J.D., Bowen, V., Dupuis, P., Noftall, F., (1988).
Manipulation and mobilization of the third meta-carpophalangeal joint.
Manual Med. 3, 135-150.Pratt-Thomas, H.R., Beyer, K.E., (1947).
Cerebellar and spinal injuries after chiropractic manipulation.
Journal of American Medical Association 133, 600-603.Reggars,J.W., (1996).
Recording techniques and analysis of the articular crack.
Australasian Chiropractic and Osteopathy 5(3), 86-92.Sandoz, R., (1969).
The significance of the manipulative crack and of other articular noises.
Ann.SwissChiro.Assoc. 4,47-68.Symons, B.,Leonard, T.R.,Herzog, W., (2002).
Internal Forces Sustained by the Vertebral Artery During Spinal Manipulative Therapy
J Manipulative Physiol Ther 2002 (Oct); 25 (8): 504–510Terrett,A.G.J., Kleynhans,A.M., (1980).
Cerebrovascular complications of manipulation.
In: Haldeman, S.(Ed.), in Principles and Practice of Chiropractic, second edn.
Appleton & Lange, Connecticut, pp. 579-598.Triano,J.,Schultz,A.B., (1997).
Loads transmitted during lumbosacral spinal manipulative therapy.
Spine 22, 1955-1964.Triano,J.J., (2000).
The mechanics of spinal manipulation in Clinical Biomechanics of Spinal Manipulation.
In: Herzog, W.(Ed.). Churchill-Livingstone, Philadelphia, PA, pp.92-190.Triano,J.J.,Schultz,A.B., (1990).
Cervical spine manipulation: applied loads, motions and myoelectric responses.
Proc.14th Mtg.Amer.Soc.Biomech.14, 187-188.Wood,J., Adams,A.H., (1984).
Forces used in selected chiropractic adjustments of the lowback: A preliminary study.
The Research Forum,. Palmer College of Chiropractic 1,16-23.
Return to ABOUT SPINAL ADJUSTING
Since 10-18-2018

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |