

Evidence-Based Evaluation of Complementary Health
Approaches for Pain Management in the United StatesThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Mayo Clin Proc. 2016 (Sep); 91 (9): 1292–1306 ~ FULL TEXT
OPEN ACCESS Richard L. Nahin, PhD, MPH • Robin Boineau, MD, MA • Partap S. Khalsa, DC, PhD
Barbara J. Stussman, BA • Wendy J. Weber, ND, PhD, MPH
National Center for Complementary and Integrative Health,
National Institutes of Health,
Bethesda, MD. Electronic
NahinR@mail.nih.gov
Although most pain is acute and resolves within a few days or weeks, millions of Americans have persistent or recurring pain that may become chronic and debilitating. Medications may provide only partial relief from this chronic pain and can be associated with unwanted effects. As a result, many individuals turn to complementary health approaches as part of their pain management strategy.
This article examines the clinical trial evidence for the efficacy and safety of several specific approaches-acupuncture, manipulation, massage therapy, relaxation techniques including meditation, selected natural product supplements (chondroitin, glucosamine, methylsulfonylmethane, S-adenosylmethionine), tai chi, and yoga-as used to manage chronic pain and related disability associated with back pain, fibromyalgia, osteoarthritis, neck pain, and severe headaches or migraines.
From the FULL TEXT Article:
INTRODUCTION
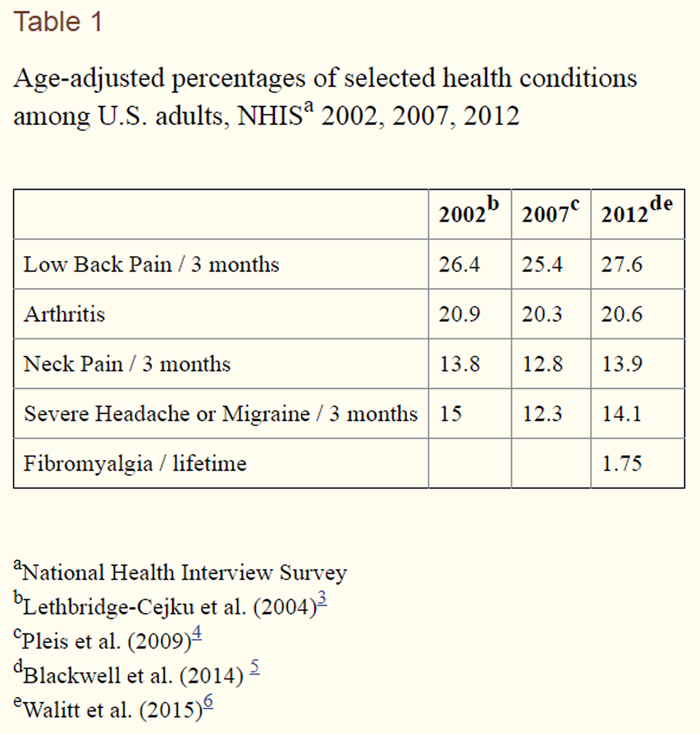
The most recent national estimate suggests that 126 million adults suffer from some pain in a given year [1] with about one-third (40 million adults) suffering from severe pain. Pain is often associated with poor general health, health-related disability and increased health care utilization. [2] Yet according to the Institute of Medicine (2011), [2] pain is routinely undertreated in health care; pain care that is provided is often fragmented, without a comprehensive assessment or treatment plan, and patients may encounter difficulty obtaining the full range of potential treatments.

Table 1
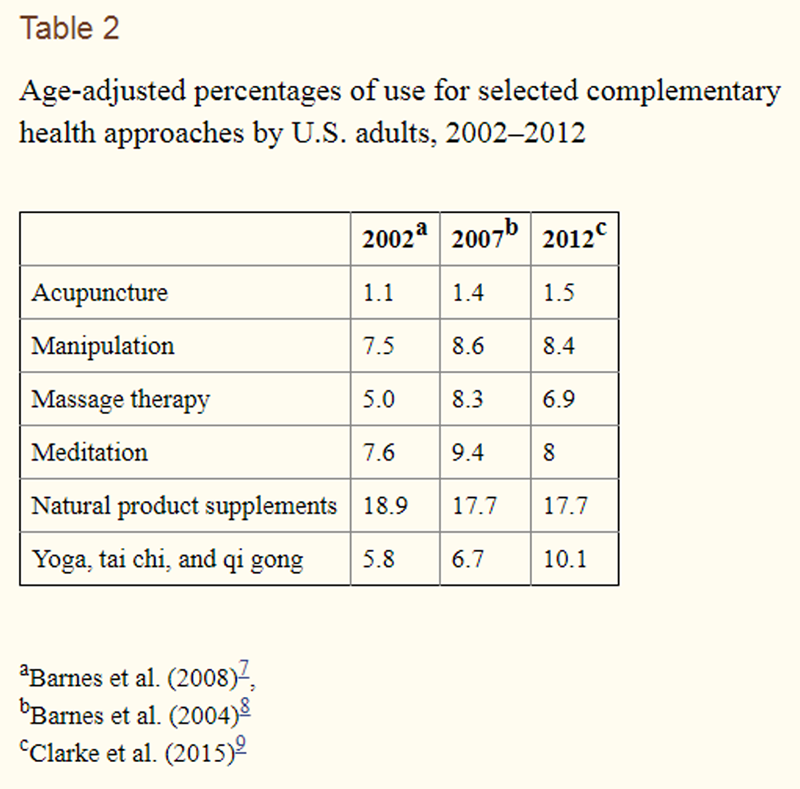
Table 2 Back pain, joint pain, neck pain and headaches are among the most common types of pain experienced by US adults (Table 1). [3–6] The prevalence rates for these conditions have remained relatively stable over time. Among the many pharmacological and non-pharmacological approaches that have been incorporated into pain management strategies are complementary health approaches. This broad category of care includes procedures by licensed providers such as acupuncturists, chiropractors, and massage therapists, as well as self-care approaches such as relaxation techniques (e.g., meditation), and meditative movement-based approaches (e.g., yoga and tai chi), as well as natural products such a glucosamine and herbal medicines. National surveys going back more than 25 years have consistently found that these complementary approaches are used by about 30% to 40% of the US public in a given year, [7–11] although use of a given approach may wax and wane over time (Table 2).
While a substantial part of this use is for overall wellness and prevention, [12, 13] painful conditions are the most common health conditions for which individuals turn to these complementary approaches. [7, 8, 10, 11, 14] In 2007, for example, about 14.3 million adults used a complementary health approach for their back pain, while about 5.0 million used these approaches for their neck pain, and 3.1 million for their arthritis. [7] Far fewer individuals used complementary health approaches for other chronic diseases such as depression (1.0 million), hypertension (0.8 million), diabetes (0.7 million) or cancer (0.4 million).
Based on national survey data, [14] this high use of complementary health approaches for painful conditions translated into $8.5 billion out-of-pocket for these approaches to manage back pain, $3.6 billion to manage neck pain, and $2.3 billion to manage arthritis. Substantially less is spent out-of-pocket on complementary health approaches to treat other chronic health conditions such as depression ($1.1 billion), hypertension ($0.7 billion), diabetes ($0.3 billion), and cancer ($0.2 billion).
Given the high use of complementary health approaches for pain, a number of specific complementary approaches have undergone mechanistic and clinical evaluations culminating in phase III trials. This article examines the clinical trial evidence for the efficacy, effectiveness and safety of several widely used approaches – acupuncture, manipulation, massage therapy, relaxation techniques including meditation, selected natural product supplements (e.g., chondroitin and glucosamine) tai chi, and yoga (defined in Supplemental Appendix 1) – as used to manage chronic pain and related disability associated with back pain, osteoarthritis, neck pain, and severe headaches or migraines, conditions frequently seen and managed in the primary care setting. Fibromyalgia was included in this review as an example of a complex pain syndrome that is often managed with a multi-modal approach that may include complementary approaches. Cancer pain is certainly a major public health concern but is more likely to be addressed outside of the primary care setting (e.g., by oncologists, at cancer centers, as part of palliative care, etc.).
The randomized, controlled clinical trial (RCT) is considered the strongest study design for investigating the efficacy, effectiveness and safety of pharmacological, behavior, and physical interventions. To identify examples of RCT’s for each complementary approach, we performed searches of the MEDLINE database for articles published from 1966 through March, 2016 using the search strategy outlined in Supplemental Appendix 2. In order to make this review as relevant as possible to the primary care provider in the US, we limit this review to RCT’s either done in the US or that included participants from the US. This decision is based on two factors. First, the unique health care system in the US versus other countries means that the standard care or usual care control groups used in the US and other countries may vary substantially. Thus whether or not a given complementary approach performs better than usual care in another country may not reflect how the approach would perform in US trials. Another factor is that the training and licensure of acupuncturists, chiropractors and naturopathic doctors vary substantially among countries, as does the marketing, regulation and use of dietary supplements. For instance, in Germany, the location of some of the largest acupuncture trials, acupuncture is only practiced by medical doctors, while the vast majority of acupuncture treatment in the US is provided by licensed acupuncturists. Thus, the findings from German trials may not be directly comparable to acupuncture as practiced in the US.
Brief summaries of the reviewed RCTs are presented below with details provided in online Supplemental Tables. The findings of these RCTs also illustrate several methodological issues that should be considered when interpreting the trial data. These issues are summarized briefly at the end of this article.
LOW BACK PAIN
Acupuncture
We found four RCT’s (total participants = 1,092) [15–18] that assessed the clinical benefit of acupuncture for treatment of low back pain (LBP) (age range: 28–60, mostly white race), and used primary study outcomes of self-report of pain intensity (numeric rating scale [NRS] or visual analog scale [VAS]) and/or functional disability (Roland-Morris Disability Questionnaire [RMDQ], Oswestry Disability index [ODI], or Disability Rating Index). Cherkin et al. (2001 [15] & 2009 [16]) both reported modest improvement in pain intensity and function compared to usual care. In pregnant women using auricular acupuncture, Wang et al. (2009) [17] found a significant reduction in pain intensity and function compared to no treatment control. Comparison of verum- to sham-acupuncture had mixed results with two RCTS [16, 18] finding no significant difference and 1 RCT [17] finding a slight but significant difference. No significant adverse events were reported.
Massage Therapy
We summarize seven RCTs studying the use of massage for LBP [15, 19–25] (total participants = 829). Massage types included Swedish/relaxation, structural, structural integration, and muscle energy; sessions varied in duration from 15 – 90 minutes. For chronic LBP (cLBP), 2 larger studies [15, 19] reporting massage compared to usual care resulted in modest improvements in pain and function at 10 weeks, but the benefit was not sustained at 52 weeks. [15] Three smaller studies compared massage to either usual outpatient rehabilitation [24] or relaxation [22, 23] and did not observe significant between-group differences for pain and/or function. For acute or subacute LBP, 2 smaller studies found significant, albeit modest, improvements in pain compared to no treatment (–1.5 pts. NRS) [21] or function (–18% ODI) [25] compared to a putative placebo. No RCTs reported significant adverse events.
Osteopathic Manipulative Therapy
Six RCTs of osteopathic manipulative therapy (OMT) for LBP are reviewed (total participants = 1308). [26–31] 2 RCTs examined OMT compared to sham-OMT for cLBP [30, 31] using similar intervention paradigms and reported mixed results with 1 not finding any significant difference and 1 showing a –9mm reduction in pain intensity (VAS). 2 RCTs compared OMT to usual care for acute or subacute LBP [26, 27] and both reported no significant improvement for function/disability but mixed results for pain intensity for between-group differences. In pregnant women with LBP, 2 studies compared the benefit of adding OMT or a placebo-ultrasound to usual obstetric care, and reported significant, modest improvements with added care but no significant between-group differences. [28, 29] No RCTs reported significant adverse events.
Spinal Manipulation
We reviewed 24 RCTs [32–55] (total participants = 4,503, all adults) of spinal manipulation (SM) for LBP. Recent data suggest that for cLBP, the “dose” of SM (defined as the # of sessions) may affect outcomes, [45, 46, 56] and hence the dose utilized was dichotomized for this report depending upon whether 6+ sessions of SM were provided in a given study. No RCTs reported significant adverse events.Chronic LBP There were 9 studies of SM for cLBP (total participants = 1,882), [32, 35–37, 40, 44–46, 50] 8 of which employed 6+ sessions for treatment, and 1 of these studies was principally (> 2/3) of adult women. [32] For the 4 larger RCTs (each with 200+ participants) [37, 44, 46, 50] that compared HVLA-SM to an active comparison (exercise, usual care, physical therapy, light touch), 3 found significant, albeit modest, between-group differences for pain intensity and/or function. 2 studies directly examined dose of HVLA-SM [45, 46] and both found the higher doses (12 and 18 sessions of SM) provided larger improvement at 12 and 52 weeks, respectively. 1 RCT utilized a putative placebo-SM [32] and found that after the first session that verum-SM > sham-SM > no treatment, but at 2 weeks, there were no significant between-group differences. 1 RCT compared thrust to non-thrust SM [40] (less than 6 sessions) and reported no significant between-group differences.
Acute, sub-acute, or mixed LBP There were 15 studies of SM for either acute, subacute, or a mixture of types of LBP (total participants = 2,621). [33, 34, 38, 39, 41–43, 47–49, 51–55] Six of these studies were of modest – moderate size (i.e., > 100 participants) and utilized 6+ sessions of SM. [38, 42, 49, 51, 53, 54] The results of these studies were mixed with some demonstrating modest, significant benefit of SM compared to active intervention (physical therapy, back school, medication, usual care) at ~4 weeks for pain intensity and/or function, [42, 49, 54] but others not reporting significant between-group differences. [38, 51, 53] 1 RCT examined pregnant women with LBP [42] and found that adding SM + exercise to usual obstetric care provided modest improvement in pain and function/disability.
There were 5 studies of SM for either acute and/or subacute LBP that used less than 6 treatment sessions, [33, 39, 41, 47, 55] but only 1 of these (and the largest) was an effectiveness study: Fritz et al. (2015) [41] did a RCT of 4 sessions over 4 weeks of SM + exercise vs. usual primary care and found at 3 months significant between-group improvement in function (–3.2 pts ODI). The other 4 studies (sample sizes ranged from 54 – 123) compared different types of SM and/or SM to an active intervention (e.g., exercise). In general, these 4 studies reported that all groups improved and there were very small or no significant between-group differences; though it is unclear whether these 4 studies were sufficiently powered to definitively ascertain whether differences existed.
There were 4 studies of SM that by design had mixed LBP [34, 48, 52, 53] (i.e., the inclusion criteria allowed participants with acute, sub-acute, or chronic LBP; 3 of these studies utilized 6+ treatment sessions. All studies had 1 or more active comparison groups (e.g., massage, electrical stimulation, usual care, steroid injection, physical therapy), and in all studies, all groups improved but there were no significant between-group differences.Yoga
Six RCTs of yoga for cLBP [57–62] are examined (total participants = 596, all adults, predominantly female). Three named forms of yoga were studied: hatha, [57, 58] viniyoga, [59, 60] and Iyengar; [61, 62] all were done in group settings, with class durations from 60 – 90 minutes, and number of sessions ranging from 12 – 24, either once or twice per week, with recommendations for home practice. Compared to usual care, 2 studies [59, 60] found yoga provided improvements in pain bothersomeness and function, but the results were mixed when compared to exercise/stretching. A dose-response study [57] compared 1/week to 2/week classes and found both had equivalent improvements in pain intensity and function. 3 smaller studies compared yoga to wait-list [58, 61] or education control [62] and reported significant, modest reductions in pain intensity and function/disability. No RCTs reported significant adverse events.
Additional information on all back pain RCT’s can be found in Supplemental Table 1.
FIBROMYLGIA
All trials we reviewed for fibromyalgia used the 1990 American College of Rheumatology (ACR) classification criteria [63] except for one [64] that used an older definition.
Acupuncture
Four RCT’s examined acupuncture versus sham acupuncture for pain, physical function, global well-being, sleep, fatigue, and adverse events. [65–68] Martin et al. (2006) [68] found a significant improvement between the electro-acupuncture versus a sham electro-acupuncture control group. Differences were seen on the Fibromyalgia, Impact Questionnaire (FIQ), on fatigue and on anxiety. No other trial found significant differences between groups on any outcome. There were no serious adverse events reported in any of these studies. In one study, minor adverse events (e.g. discomfort at site of needle insertion or simulation of needles) were reported by 89% of participants. [65]
Relaxation Techniques
Two studies (93 total participants, mostly female and white) looked at biofeedback versus control groups (attention control and placebo) as a treatment for symptoms of fibromyalgia. [64, 69] Buckelew et al. (1998) [64] saw a significant improvement in the Tender Point Index in the biofeedback group versus an attention control but not for any other outcome measure. Nelson et al. (2010) [69] did not find any differences between biofeedback and a placebo biofeedback. A small study (90 women) found that MBSR significantly reduced perceived stress, sleep disturbance, and lessened the severity of symptoms in persons with fibromyalgia versus a waitlist control group. [70] Another RCT examined the effects of Affective Self-Awareness, a technique that places primary importance on the awareness and expression of emotions underlying fibromyalgia symptoms, on 45 women with fibromyalgia, and found significant pain reduction and improved physical functioning versus a waitlist control group. [71]
Astin et al. (2003) [72] examined the effects of an intervention combining mindfulness meditation and qi gong and found that the combined intervention was no better than an educational/support control group for pain, depression, and physical functioning. Two studies [73, 74] (112 total participants, mostly female) examined guided imagery versus usual care control as a treatment for symptoms of fibromyalgia. One study [74] found a significant decrease in the FIQ compared to the usual care control group. The second study [73] found positive effects of guided imagery on pain intensity, fatigue, and depression versus the control group. Both studies found improvements in self-efficacy for managing symptoms. Only one study [69] reported on adverse events and there were none noted.
Massage
A small study (12 women) examined Swedish massage versus myofascial release therapy for fibromyalgia symptoms. [75] No difference was seen between groups on the FIQ.
Tai Chi
A study of 98 adults with fibromyalgia, aged 40 and over, mostly white and female, compared Yang style tai chi (modified for fibromyalgia patients) with an educational control and found that the tai chi group had a greater decrease in the FIQ. [76] Another study (59 adults with fibromyalgia) compared Yang style tai chi to a control combining wellness education and stretching classes, and found that the tai chi group had greater improvement in the FIQ. [77]
Yoga
A small study (53 women) looked at yoga versus waitlist for management of fibromyalgia symptoms and found that those practicing yoga had significant improvement in the FIQ. [78] No adverse events were noted.
Additional information on all fibromyalgia RCT’s can be found in Supplemental Table 2.
NECK PAIN
Massage
Four randomized controlled trials examined whether massage could relieve symptoms associated with chronic neck pain. [79–82] One study did not report patient demographics, the others studied subjects ages 20 to 64. Primary outcomes included The Neck Disability Index (NDI), an 11 point neck bothersome score, the VAS pain scale, and range of motion (ROM). Sherman et al. (2009) [81] found significant improvement on the NDI for those randomized to 10 massage therapy session over 10 weeks versus those assigned to a self-care book on managing neck problems. In an RCT by Field et al., [80] individuals were randomized to either a wait list control, or 30 minutes of massage therapy weekly for 4 weeks combined with daily self-massage. At the completion of the intervention, those assigned to massage therapy showed improvements in pain and range of motion compared to the control group. Sherman et al. [82] demonstrated a dose response relationship between the number and duration of message sessions per week and improvement in the NDI and neck pain intensity.
The findings indicated that 60 minutes of massage for 2 to 3 times per week was significantly better than either 30 or 60 minutes of massage once per week after the 4 weeks of treatment. In a follow-up to Sherman et al. (2014), [82] Cook et al. (2015) [79] re-consented and randomized participants to one additional massage therapy session per week for 6 additional weeks. Those randomized to the booster sessions had significantly improved pain and function verses those that did not receive the booster at the end of treatment; the difference between groups was no longer significant after 14 weeks of follow-up.
Spinal manipulation
We reviewed three randomized trials of spinal manipulation for neck pain. [83–85] One study assessed manipulation compared to mobilization with a 2×2×2 factorial design: with or without heat, or with or without electrical muscle stimulation (EMS); [84] no significant differences in outcomes were seen between groups. Evans et al. [83] compared spinal manipulation combined with supervised exercising to supervised exercising alone and also to home exercise. After completion of the 12–week intervention, no difference was seen between spinal manipulation combined with supervised exercising and supervised exercising alone; however, both these groups showed significant improvement in neck pain versus only home exercise.
Maiers et al. [85] assessed the efficacy of three groups: 1) manipulation plus home exercise; 2) versus supervised rehabilitation exercise plus home exercise; and 3) home exercise alone. Spinal manipulation with home exercise produced significantly better reduction in pain than home exercise alone. No significant difference was seen between manipulation and home exercise, versus supervised rehabilitation exercise plus home exercise.
There was one RCT of manual cervical distraction, [86] a traction-based therapy with low, medium, and high forces assessed. The goal of the study was to identify a viable sham-control (see Supplemental Table 3 for details). The study endpoints included pain VAS, NDI, and credibility and expectancy questionnaire. The investigators did report benefit in medium or high force interventions.
Additional information on all neck pain RCT’s can be found in Supplemental Table 3.
OSTEOARTHRITIS OF THE KNEE
Acupuncture
Four RCT’s examined whether acupuncture needling could relieve symptoms associated with osteoarthritis of the knee. [87–90] These studies used similar definitions of knee OA. Participants were predominately female; had mean ages between 60 and 65; and had knee pain for an average of 9 to 11 years. All studies incorporated either the Western Ontario and McMaster Universities (WOMAC) arthritis Index total score or the WOMAC pain subscore as the primary outcomes. In two of the trials, [89, 90] no difference was seen between verum acupuncture and sham acupuncture for either the primary or secondary outcome measure. The third trial [87] using a sham control saw significantly better improvement in both the WOMAC pain subscale and function subscale after 14 weeks of treatment. For the three trials that also incorporated either an attention control [87] or standard care controls, [88, 90] verum acupuncture produced significantly better improvement in primary and secondary outcomes than did the control group. Across trials, adverse events associated with acupuncture were few in number with the most common complaints being pain at the needling site and muscle soreness that resolved soon after the treatment session ended.
Glucosamine and Chondroitin
We reviewed eight RCT’s examining the efficacy of two dietary supplements, glucosamine and/or chondroitin, in individuals with knee OA. [91–98] These studies varied substantially in how knee OA was defined, as well as in the primary outcome measures used (see Supplemental Table 4).
Three different configurations of glucosamine were used: glucosamine hydrochloride (HCl), [93–95] glucosamine sulfate, [91, 92, 98] and glucosamine bound to a polymer. [97] One trial did not identify the configuration of glucosamine. [96] Doses of glucosamine varied from 1000 mg per day for 6 weeks [98] to 1500 mg per day for 24 weeks. [91, 95] Chondroitin sulfate was studied in two trials at a dose 1200 mg/day for 6 months [91, 95] and in one trial at the same dose but for 8 weeks. [93]
All studies employed a placebo control group. Participants in two trials were made up exclusively [93] or predominately of males; [96] participants in four other trials were predominately females; [91, 94, 95, 98] the remaining two trial were closely balanced in men and women. [92, 97] Mean participant ages for the trials varied from 45 years of age [91] to 72 years of age. [95]
Mixed results were found in trials comparing glucosamine versus a placebo control with pain relief or functional improvement as the primary outcomes. Three trials found glucosamine superior to placebo, [92, 97, 98] and three trials failed to see a difference between groups. [91, 94, 96]
Mixed results were seen in the three trials studying a combination of glucosamine and chondroitin. Leffler et al. [93] found that a combination of glucosamine HCl and chondroitin sulfate (and manganese acerbate) was superior to placebo for providing pain relief. In two other trials, the combination of glucosamine (either sulfate or HCl) and chondroitin sulfate were no better than placebo for either pain relief or function. [91, 95]
Across trials, adverse events were generally mild (gastrointestinal distress being the most common) with no differences seen between those taking glucosamine or chondroitin and those taking placebo.
Massage therapy
Two RCT’s studied the efficacy of Swedish massage therapy for symptoms associated with osteoarthritis of the knee. [99, 100] The two studies were similar in that both:1) defined knee OA using the American College of Rheumatology criteria; [101]
2) required a baseline score of at least 40 on the visual analog pain scale;
3) participants were predominately white females.In the earlier study [100], after completing the 8 week intervention, participants in the massage group saw significant improvement versus those randomized to Usual Care in the WOMAC Arthritis Index, as well as in each of the WOMAC subscales: pain, function and joint stiffness. In a dosing study, [99] individuals were randomized to one of five groups for 8 weeks:
1) Usual care;
2) 240 minutes of massage over 8 weeks;
3) 360 minutes of massage;
4) 480 minutes of massage; and
5) 600 minutes of massage.
Only individuals receiving at least 480 minutes of massage therapy (groups 4 and 5), saw substantial improvement in the WOMAC OA index and the WOMAC Pain subscale versus the Usual Care group. Across the two trials only one adverse event, discomfort at the knee in one participant, was noted.Methylsulfonylmethane (MSM)
One RCT compared MSM (6 grams/day for 12 weeks) to a placebo control. [102] Knee OA was based on ACR criteria. [101] Outcome measures were the WOMAC arthritis subscales for pain, function, and stiffness. Individuals randomized to MSM saw significant improvement in both the WOMAC pain and functions scales. However, the authors cautioned that the differences between groups were small (<20%) and probably not clinical meaningful. No difference in adverse events was seen between groups.
S-Adenoysl methionine (SAMe)
One RCT compared the dietary supplement SAMe (1200 mg/day) to celecoxib (200 mg/day for 16 weeks in a cross-over design that included a one-week washout period. [103] Knee OA was defined based on ACR criteria:102 the population was primarily female and white. The primary outcomes were VAS pain scores, WOMAC arthritis subscales for pain, function, and stiffness, and clinician assessments of OA severity. By the end of the trial, no differences were seen between the two treatment arms on any of the outcomes measures. However, the sample size was insufficient to establish equivalency. Overall adverse events were less common in those taking SAMe then those taking celecoxib.
Tai Chi
We reviewed four RCT’s that examined the efficacy of Tai Chi in those with confirmed knee osteoarthritis using various criteria for diagnosis. [104–107] The four RCT’s had similar study populations, primarily white and female, with mean ages ranging from 65 to 79. Mean BMI was also similar across studied ranging from 27.8 to 30.
In Hartman et al., [105] participants randomized to a Yang style tai chi group had significant improvement in the Arthritis Self-Efficacy scale versus those in the Routine Care group. The remaining trials compared tai chi to attention controls. [104, 106, 107] All found that Tai Chi (either Yang style or Sun Style) did better than the attention control group on both primary and secondary outcomes. Across trials the most common adverse event associated with Tai Chi was minor muscle soreness that resolved after a few days.
Yoga
Park et al. [108] completed a quasi-experimental trial, with participants randomized to either sitting yoga or Reiki; however the attention control group was chosen as a convenience sample from other participants meeting the inclusion/exclusion criteria. The primary outcome measures were the WOMAC Arthritis Index score and the pain, function, and stiffness subscales. The mean age of participants was 80, with 68.7% being male. Individuals randomized to yoga, had substantially better reduction in the WOMAC function then either the Reiki group or the attention control group (p<0.02). No other differences were seen between the three groups. No adverse advents were reported for any of the groups in this study.
Additional information on all osteoarthritis RCT’s can be found in Supplemental Table 4.
SEVERE HEADACHE AND MIGRAINE
The majority of studies we reviewed defined cervicogenic headache, migraine, and tension-type headache with the International Classification of Headache Disorders second edition. [109, 110]
Acupuncture
Coeytaux et al. [111] randomized patients with chronic daily headache to management by a neurologist with or without acupuncture. The acupuncture group had significantly reduced headache impact test scores versus the control, but there were no significant differences on pain severity.
Massage
One small study that compared myofascial trigger point massage, a sham device, and waitlist; found massage reduced headache frequency but did not significantly reduce intensity or duration of headaches. [112]
Omega-3 Fatty Acids
One study randomized adolescents with migraine to omega-3 or placebo in a cross-over study. [113] Adolescents experienced a reduction in headache frequency when taking either fish oil or placebo, but there was no significant difference between the treatments. Another study randomized patients with chronic headaches to increased omega-3 and lower omega-6 fatty acids in the diet or to lower omega-6 fatty acids in the diet. [114] The participants on high omega-3 and low omega-6 diet had greater improvement on the Headache Impact Test and number of headache days.
Relaxation techniques
Six trials we reviewed evaluated stress management, relaxation, or biofeedback for headache disorders. [115–120] Slavin-Spennyt et al. [120] randomized students with chronic headache to expression training, relaxation training, or waitlist. Both active treatments showed significant decreases in headache frequency versus the waitlist control, but did not differ among themselves. Two trials examined complementary approaches to either tension headaches or migraine. [116, 117] D’Souza et al. (2008) [117] randomized students to relaxation training, written emotional disclosure, or neutral writing. The relaxation group had greater reductions in headache frequency and the associated headache disability compared to the other two groups. Devineni et al. [116] randomized participants to an internet behavioral intervention or a waitlist. The behavioral intervention demonstrated improvement in the headache index versus waitlist.
A trial randomized children with migraine to hand warming biofeedback with stress management, hand cooling biofeedback (attention control), or waitlist. [119] The warming biofeedback group had improved headache index scores compared to the other groups. Holroyd et al. [118] randomized participants with chronic tension headache to tricyclic antidepressant, placebo, stress management, or stress management plus tricyclic antidepressant. Both the medication and stress management groups had improvements over placebo, but the combination produced the best outcomes. Blanchard et al. [115] randomized patients with headache to biofeedback with relaxation training, biofeedback plus cognitive therapy, sham meditation, or a headache monitoring control condition. All of the treatment groups including the “sham” meditation group had improvements in the headache index in comparison to the monitoring control group.
Spinal and Osteopathic Manipulation
One trial randomized patients with chronic cervicogenic headache to two doses of spinal manipulation or light massage; [121] based on the literature, the light massage should have little, if any, specific effects and was therefore chosen as a control for time and physical contract with the patient. Haas and colleagues found improvement over all time points favoring spinal manipulation compared to light massage and a dose effect with the spinal manipulation. Two RCT’s were identified that assessed manipulation in individuals with tension headache. [122, 123] The first trial randomized patients with chronic tension type headache to spinal manipulation or amitriptyline medication and found no differences between the groups; [122] however the trial did not appear powered to detect non-inferiority.
The second study was a small trial that randomized patients to osteopathic manipulation, a palpation examination, or no treatment. [123] Authors noted an improvement in headache severity for the spinal manipulation group; however no statistical comparisons were made between groups. Nelson and colleagues study randomized patients with migraine to amitriptyline, spinal manipulation, or both treatments. [124] The study found no significant differences between the groups; however it did not appear that the trial was powered to detect non-inferiority (see Supplemental Table 5).
Additional information on all headache RCT’s can be found in Supplemental Table 5.
OVERALL SUMMARY OF RCT DATA
Table 3
Table 4 Tables 3 (Efficacy), and 4 (Effectiveness) provide concise summaries of the reviewed clinical trial data for each complementary approach across painful health conditions. In these tables, positive trials are those in which the complementary approach provided statistically significant improvements in pain severity or pain-related disability or function compared to the control group. Negative trials are those in which no difference was seen between groups. Based on a preponderance of positive trials versus negative trials, current evidence suggests that the following complementary approaches may help some patients manage their painful health conditions:
Acupuncture and Yoga for back pain;
Acupuncture and Tai Chi for osteoarthritis of the knee;
Massage therapy for neck pain with adequate doses and for short term benefit; and
Relaxation techniques for severe headaches and migraine.Weaker evidence suggests that Massage therapy, Spinal Manipulation and Osteopathic Manipulation might also be of some benefit to those with Back Pain, while Relaxation approaches and Tai Chi might help those with Fibromyalgia.
SAFETY
Generally the reporting of safety data in the reviewed RCTs was minimal. For those trials that did report safety data, we have summarized this information in the text for each painful health condition. In no case did an RCT identify a serious adverse event associated with any of the complementary approaches examined. The most common adverse events (gastrointestinal distress) were noted in trials of dietary supplements (glucosamine, chondroitin, MSM, SAMe). In some trials, tai chi and yoga were associated with minor muscle or joint soreness, and acupuncture was associated with minor pain and/or bruising at the needling site.
Comparisons to recent systematic reviews
Our search criteria identified a number of recent (2010 or later) systematic reviews that covered our topics of interest. [125–133] Conclusions from these systematic reviews for practitioner approaches (acupuncture, chiropractic, massage therapy) [125–131] and dietary supplements [132] were generally consistent with our findings. For instance, in a comprehensive reviews of both pharmacological and non-pharmacological approaches to manage back pain, Chou et al. (20016) [125] found that acupuncture and yoga appear to be effective for improving pain and/or function in back pain. A Cochrane systematic review concluded that acupuncture was a viable treatment option for osteoarthritis of the knee. [127] Also concurring with the present analysis, the meta-analysis by Deare et al. [126] concluded that acupuncture was not an effective therapy for pain or function in individuals with Fibromyalgia. In their systematic review, Posadzki and Ernst [128] found little data supporting the use of spinal manipulation for headaches.
Supporting our conclusions is a recent comprehensive meta-analysis of trials studying glucosamine for osteoarthritis, [132] which found considerable variability in results across trials and concluded that neither glucosamine sulfate or HCl provide pain relief. The RCT’s examined in two systematic reviews of yoga for arthritis [129, 130] overlapped considerably with RCTs in the present review. The authors of the systematic reviews concluded that yoga appears to be a viable option for relieving pain and discomfort associated with arthritis, but that larger, better designed trials were needed. A recent systematic review [131] that included international trials found that “clinically relevant effects of OMT were found for reducing pain and improving functional status” for those with back pain. Although this is a stronger conclusion than we reached, the authors’ identified deficiencies in trial methodology and called for larger, better quality RCT’s to provide firm conclusions.
Not all recent systematic reviews agreed with our conclusions. A recent Cochrane Collaboration meta-analysis [133] concluded that spinal manipulation was no more effective than “inert” interventions for managing back pain and related disability. However this review only included RCT’s published through 2009. We reviewed eight RCTs published since then. Of these, two were negative trials32,27 and six were positive trials. [36, 41–43, 46, 54] Inclusion of these trials into the meta-analysis might have lead Rubenstein et al. [133] to draw a different conclusion.
Caveats
A number of methodological issues temper our conclusions:1) The trial samples tend to be white, female and older, with very few, if any minority group participants; as such the generalizability of the findings to the breath of patients seen by primary care providers in the U.S. is still unresolved;
2) Often the trials reviewed were small, with fewer than 100 total participants. Small trials are prone to more variability and to false-negative results.
3) In many of the trials where the statistical superiority of a given complementary health approach was demonstrated, it was not clear if the differences versus the control group were clinically relevant;
4) For the given painful health condition, a wide number of outcome measures were often used to asses pain and function; this plethora of outcomes may partly explain the conflicting results seen across trials;
5) For most complementary approaches there are no standard treatment protocols or algorithms, or in the case of dietary supplements, no rigorously established dosages and products; as such, trials of a given complementary approach rarely compare the exact same intervention; and
6) Our findings that relatively few mild adverse events and no serious adverse events were associated with complementary approaches is consistent the findings from a number of systematic reviews.125–133However, even large clinical trials are not powered to identify infrequent adverse events; therefore, it is likely that this review is underestimating the entire range of events associated with the complementary approaches examined. Finally, our review was intended to be an overview of data from RCTs performed in the US. The inclusion of RCTs performed outside the US may have resulted in a different set of recommendations.
Supplementary Material
Supplemental Appendix 1
Descriptions of complementary health approaches.
Supplemental Table 1
Summary of U.S. randomized controlled trials examining the use of complementary health approaches for back pain.
Supplemental Table 2
Summary of U.S. randomized controlled trials examining the use of complementary health approaches for Fibromyalgia.
Supplemental Table 3
Summary of U.S. randomized controlled trials examining the use of complementary health approaches for neck pain.
Supplemental Table 4
Summary of U.S. randomized controlled trials examining the use of complementary health approaches for osteoarthritis of the knee.
Supplemental Table 5
Summary of U.S. randomized controlled trials examining the use of complementary health approaches for severe headache or migraine.List of abbreviations
ACR = American College of Rheumatology
cLBP = chronic low back pain
EMS = electrical muscle stimulation
FIQ = Fibromyalgia Impact Questionnaire
HVLA-SM = high velocity, low amplitude, spinal manipulation
LBP = low back pain
MSM = Methylsulfonylmethane
NDI = Neck Disability Index
NRS = numeric rating scale
OA = osteoarthritis
ODI = Oswestry Disability index
OMT = osteopathic manipulative therapy
RCT = randomized clinical trial
RMDQ = Roland-Morris Disability Questionnaire
ROM = range of motion
SAMe = S-Adenoysl methionine
SM = spinal manipulation
VAS = visual analog scale
WOMAC = Western Ontario and McMaster Universities Arthritis Index
Financial support and conflict of interest disclosure:
The authors performed this work as part of their official federal duties. No outside financial support was provided. The authors have no competing interests.
References:
Nahin RL.
Estimates of pain prevalence and severity in adults: United States, 2012.
J Pain. 2015;16(8):769–780Institute of Medicine (IOM)
Relieving Pain in America: A Blueprint for Transforming Prevention,
Care, Education, and Research
Washington, DC: The National Academies Press, 2011.Lethbridge-Cejku M, Schiller JS, Bernadel L.
Summary health statistics for U.S. adults:
National Health Interview Survey, 2002.
Vital Health Stat. 2004;222:1–151Pleis JR, Lucas JW.
Summary health statistics for U.S. adults:
National Health Interview Survey, 2007.
Vital Health Stat. 2009;10(240):1–159Blackwell DL, Lucas JW, Clarke TC.
Summary health statistics for U.S. adults:
national health interview survey, 2012.
Vital Health Stat. 2014;260:1–161Walitt B, Nahin RL, Katz RS, et al.
The Prevalence and Characteristics of Fibromyalgia in
the 2012 National Health Interview Survey.
PLoS One. 2015;10(9):e0138024Barnes PM , Bloom B , Nahin RL:
Complementary and Alternative Medicine Use Among Adults and Children:
United States, 2007
US Department of Health and Human Services,
Centers for Disease Control and Prevention,
National Center for Health Statistics, Hyattsville, MD, 2008.Barnes PM , Powell-Griner E , McFann K , Nahin RL:
Complementary and Alternative Medicine Use Among Adults:
United States, 2002
Advance Data 2004 (May 27); 343: 1–19Black, LI, Clarke, TC, Barnes, PM, Stussman, BJ, and Nahin, RL.
Use of Complementary Health Approaches Among Children Aged 4–17 Years
in the United States: National Health Interview Survey, 2007–2012
National Health Statistics Report 2015 (Feb 10); (78): 1–19Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van Rompay M, Kessler RC.
Trends in Alternative Medicine Use in the United States, 1990 to 1997:
Results of a Follow-up National Survey
JAMA 1998 (Nov 11); 280 (18): 1569–1575Eisenberg DM, Kessler RC, Foster C. et al.
Unconventional Medicine in the United States:
Prevalence, Costs, and Patterns of Use
New England Journal of Medicine 1993 (Jan 28); 328 (4): 246–252Stussman BJ, Black LI, Barnes PM, et al.
Wellness-related Use of Common Complementary Health Approaches
Among Adults: United States, 2012
National Health Statistics Report 2015 (Nov 4); (85): 1–12Upchurch DM, Rainisch BW.
The importance of wellness among users of complementary and
alternative medicine: findings from the
2007 National Health Interview Survey.
BMC Complement Altern Med. 2015;15:362–372Nahin RL, Stussman BJ, Herman PM.
Out-Of-Pocket Expenditures on Complementary Health Approaches
Associated With Painful Health Conditions in a
Nationally Representative Adult Sample.
J Pain. 2015;16(11):1147–1162Cherkin DC, Eisenberg D, Sherman KJ, et al.
Randomized trial comparing traditional Chinese medical acupuncture,
therapeutic massage, and self-care education for chronic low back pain.
Arch Intern Med. 2001;161(8):1081–1088Cherkin DC, Sherman KJ, Avins AL, et al.
A randomized trial comparing acupuncture, simulated acupuncture,
and usual care for chronic low back pain.
Arch Intern Med. 2009;169(9):858–866Wang SM, Dezinno P, Lin EC, et al.
Auricular acupuncture as a treatment for pregnant women who have
low back and posterior pelvic pain: a pilot study.
Am J Obstet Gynecol. 2009;201(3):271.e271–279Wasan AD, Kong J, Pham LD, et al.
The impact of placebo, psychopathology, and expectations
on the response to acupuncture needling in patients
with chronic low back pain.
J Pain. 2010;11(6):555–563Cherkin DC, Sherman KJ, Kahn J, et al.
A comparison of the effects of 2 types of massage and usual care
on chronic low back pain: a randomized, controlled trial.
Ann Intern Med. 2011;155(1):1–9Eisenberg DM, Post DE, Davis RB, et al.
Addition of choice of complementary therapies to usual care
for acute low back pain: a randomized controlled trial.
Spine (Phila Pa 1976) 2007;32(2):151–158Field T, Figueiredo B, Hernandez-Reif M, et al.
Massage therapy reduces pain in pregnant women, alleviates
prenatal depression in both parents and improves their relationships.
J Bodyw Mov Ther. 2008;12(2):146–150Field T, Hernandez-Reif M, Diego M, et al.
Lower back pain and sleep disturbance are reduced
following massage therapy.
J Bodyw Mov Ther. 2007;11(2):141–145.Hernandez-Reif M, Field T, Krasnegor J, et al.
Lower back pain is reduced and range of motion
increased after massage therapy.
Int J Neurosci. 2001;106(3–4):131–145Jacobson EE, Meleger AL, Bonato P, et al.
Structural integration as an adjunct to outpatient rehabilitation
for chronic nonspecific low back pain: a randomized pilot clinical trial.
Evid Based Complement Alternat Med. 2015 2015813418Wilson E, Payton O, Donegan-Shoaf L, et al.
Muscle energy technique in patients with acute low back pain:
a pilot clinical trial.
J Orthop Sports Phys Ther. 2003;33(9):502–512Andersson GB, Lucente T, Davis AM, et al.
A comparison of osteopathic spinal manipulation with
standard care for patients with low back pain.
N Engl J Med. 1999;341(19):1426–1431Cruserd A, Maurer D, Hensel K, et al.
A randomized, controlled trial of osteopathic manipulative treatment
for acute low back pain in active duty military personnel.
J Man Manip Ther. 2012;20(1):5–15Hensel KL, Buchanan S, Brown SK, et al.
Pregnancy Research on Osteopathic Manipulation
Optimizing Treatment Effects: the PROMOTE study.
Am J Obstet Gynecol. 2015;212(1):108.e101–109Licciardone JC, Buchanan S, Hensel KL, et al.
Osteopathic manipulative treatment of back pain and
related symptoms during pregnancy:
a randomized controlled trial.
Am J Obstet Gynecol. 2010;202(1):43.e41–48Licciardone JC, Minotti DE, Gatchel RJ, et al.
Osteopathic manual treatment and ultrasound therapy
for chronic low back pain: a randomized controlled trial.
Ann Fam Med. 2013;11(2):122–129Licciardone JC, Stoll ST, Fulda KG, et al.
Osteopathic manipulative treatment for chronic low back pain:
a randomized controlled trial.
Spine (Phila Pa 1976) 2003;28(13):1355–1362Bialosky JE, George SZ, Horn ME, Price DD, Staud R, Robinson ME.
Spinal Manipulative Therapy-specific Changes in Pain Sensitivity
in Individuals with Low Back Pain
Journal of Pain 2014 (Feb); 15 (2): 136–148Brennan GP, Fritz JM, Hunter SJ, et al.
Identifying subgroups of patients with acute/subacute “nonspecific”
low back pain: results of a randomized clinical trial.
Spine (Phila Pa 1976) 2006;31(6):623–631Bronfort G, Evans R, Maiers M, Anderson AF.
Spinal Manipulation, Epidural Injections, and Self-care for Sciatica:
A Pilot Study for a Randomized Clinical Trial
J Manipulative Physiol Ther. 2004 (Oct); 27 (8): 503–508Bronfort G, Goldsmith CH, Nelson CF, Boline PD, Anderson AV.
Trunk Exercise Combined with Spinal Manipulative or NSAID Therapy
for Chronic Low Back Pain: A Randomized, Observer-blinded Clinical Trial
J Manipulative Physiol Ther. 1996 (Nov); 19 (9): 570–582Bronfort G, Hondras MA, Schulz CA, Evans RL, Long CR et al (2014)
Spinal Manipulation and Home Exercise With Advice for Subacute
and Chronic Back-related Leg Pain:
A Trial With Adaptive Allocation
Annals of Internal Medicine 2014 (Sep 16); 161 (6): 381—391Bronfort G, Maiers MJ, Evans RL, Schulz CA, Bracha Y, Svendsen KH, Grimm RH, Jr.:
Supervised Exercise, Spinal Manipulation, and Home Exercise for
Chronic Low Back Pain: A Randomized Clinical Trial
Spine J. 2011 (Jul); 11 (7): 585–598Cherkin, DC, Deyo, RA, Battie, M, Street, J, and Barlow, W.
A Comparison of Physical Therapy, Chiropractic Manipulation, and Provision
of an Educational Booklet for the Treatment of Patients
with Low Back Pain
New England J Medicine 1998 (Oct 8); 339 (15): 1021-1029Cleland JA, Fritz JM, Kulig K, et al.
Comparison of the effectiveness of three manual physical therapy techniques
in a subgroup of patients with low back pain who satisfy a
clinical prediction rule: a randomized clinical trial.
Spine (Phila Pa 1976) 2009;34(25):2720–2729Cook C, Learman K, Showalter C, et al.
Early use of thrust manipulation versus non-thrust manipulation:
a randomized clinical trial.
Man Ther. 2013;18(3):191–198Fritz JM, Magel JS, McFadden M, et al.
Early Physical Therapy vs Usual Care in Patients With
Recent-Onset Low Back Pain: A Randomized Clinical Trial.
JAMA. 2015;314(14):1459–1467George JW, Skaggs CD, Thompson PA, Nelson DM, Gavard JA, Gross GA.
A Randomized Controlled Trial Comparing a Multimodal Intervention and Standard
Obstetrics Care for Low Back and Pelvic Pain in Pregnancy
Am J Obstet Gynecol. 2013 (Apr); 208 (4): 295.e1-7Goertz CM, Long CR, Hondras MA, Petri R, Delgado R, Lawrence DJ, et al.
Adding Chiropractic Manipulative Therapy to Standard Medical Care
for Patients with Acute Low Back Pain: Results of a Pragmatic
Randomized Comparative Effectiveness Study
Spine (Phila Pa 1976). 2013 (Apr 15); 38 (8): 627–634Gudavalli MR, Cambron JA, McGregor M, et al.
A randomized clinical trial and subgroup analysis to compare
flexion-distraction with active exercise for chronic low back pain.
Eur Spine J. 2006;15(7):1070–1082Haas, M., Groupp, E., and Kraemer, D.F.
Dose-response for Chiropractic Care of Chronic Low Back Pain
Spine J 2004 (Sep); 4 (5): 574–583Haas M, Vavrek D, Peterson D, Polissar N, Neradilek MB.
Dose-response and Efficacy of Spinal Manipulation for Care of
Chronic Low Back Pain: A Randomized Controlled Trial
Spine J. 2014 (Jul 1); 14 (7): 1106–1116Hadler NM, Curtis P, Gillings DB, et al.
A benefit of spinal manipulation as adjunctive therapy for
acute low-back pain: a stratified controlled trial.
Spine (Phila Pa 1976) 1987;12(7):702–706Hoehler FK, Tobis JS, Buerger AA.
Spinal manipulation for low back pain.
JAMA. 1981;245(18):1835–1838Hoiriis KT, Pfleger B, McDuffie FC, Cotsonis G, Elsangak O, Hinson R, et al.
A Randomized Clinical Trial Comparing Chiropractic Adjustments
to Muscle Relaxants for Subacute Low Back Pain
J Manipulative Physiol Ther 2004 (Jul); 27 (6): 388-398Hondras MA, Long CR, Cao Y, et al.
A Randomized Controlled Trial Comparing 2 Types of Spinal Manipulation
and Minimal Conservative Medical Care for Adults 55 Years and Older
With Subacute or Chronic Low Back Pain
J Manipulative Physiol Ther. 2009 (Jun); 32 (5): 330–343Hsieh CY, Adams AH, Tobis J, et al.
Effectiveness of four conservative treatments for subacute low back pain: a randomized clinical trial.
Spine (Phila Pa 1976) 2002;27(11):1142–1148Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Belin TR, Yu F, Adams AH
A Randomized Trial of Medical Care with and without Physical Therapy
and Chiropractic Care with and without Physical Modalities for
Patients with Low Back Pain: 6-month Follow-up Outcomes
From the UCLA Low Back Pain Study
Spine (Phila Pa 1976) 2002 (Oct 15); 27 (20): 2193–2204Pope MH, Phillips RB, Haugh LD, et al.
A prospective randomized three-week trial of spinal manipulation,
transcutaneous muscle stimulation, massage and corset
in the treatment of subacute low back pain.
Spine (Phila Pa 1976) 1994;19(22):2571–2577Schneider, M, Haas, M, Glick, R, Stevans, J, and Landsittel, D.
Comparison of Spinal Manipulation Methods and Usual Medical Care for Acute and Subacute
Low Back Pain: A Randomized Clinical Trial
Spine (Phila Pa 1976). 2015 (Feb 15); 40 (4): 209–217Sutlive TG, Mabry LM, Easterling EJ, et al.
Comparison of short-term response to two spinal manipulation techniques
for patients with low back pain in a military beneficiary population.
Mil Med. 2009;174(7):750–756Nyiendo J, Haas M, Goldberg B, Sexton G.
Patient Characteristics and Physicians' Practice Activities for
Patients with Chronic Low Back Pain: A Practice-based Study
of Primary Care and Chiropractic Physicians
J Manipulative Physiol Ther 2001 (Feb); 24 (2): 92–100Saper RB, Boah AR, Keosaian J, et al.
Comparing Once-versus Twice-Weekly Yoga Classes for Chronic Low Back Pain
in Predominantly Low Income Minorities: A Randomized Dosing Trial.
Evid Based Complement Alternat Med. 2013 2013658030Saper RB, Sherman KJ, Cullum-Dugan D, et al.
Yoga for chronic low back pain in a predominantly minority population:
a pilot randomized controlled trial.
Altern Ther Health Med. 2009;15(6):18–27Sherman KJ, Cherkin DC, Erro J, et al.
Comparing yoga, exercise, and a self-care book for chronic low back pain:
a randomized, controlled trial.
Ann Intern Med. 2005;143(12):849–856Sherman KJ, Cherkin DC, Wellman RD, et al.
A randomized trial comparing yoga, stretching, and a self-care
book for chronic low back pain.
Arch Intern Med. 2011;171(22):2019–2026Williams K, Abildso C, Steinberg L, et al.
Evaluation of the effectiveness and efficacy of Iyengar
yoga therapy on chronic low back pain.
Spine (Phila Pa 1976) 2009;34(19):2066–2076Williams KA, Petronis J, Smith D, et al.
Effect of Iyengar yoga therapy for chronic low back pain.
Pain. 2005;115(1–2):107–117Wolfe F, Smythe HA, Yunus MB, et al.
The American College of Rheumatology 1990 Criteria for
the Classification of Fibromyalgia. Report of the
Multicenter Criteria Committee.
Arthritis Rheum. 1990;33(2):160–172Buckelew SP, Conway R, Parker J, et al.
Biofeedback/relaxation training and exercise interventions
for fibromyalgia: a prospective trial.
Arthritis Care Res. 1998;11(3):196–209Assefi NP, Sherman KJ, Jacobsen C, et al.
A randomized clinical trial of acupuncture compared with
sham acupuncture in fibromyalgia.
Ann Intern Med. 2005;143(1):10–19Harris RE, Tian X, Williams DA, et al.
Treatment of fibromyalgia with formula acupuncture:
investigation of needle placement, needle
stimulation, and treatment frequency.
J Altern Complement Med. 2005;11(4):663–671Harris RE, Zubieta JK, Scott DJ, et al.
Traditional Chinese acupuncture and placebo (sham) acupuncture
are differentiated by their effects on mu-opioid receptors (MORs)
Neuroimage. 2009;47(3):1077–1085Martin DP, Sletten CD, Williams BA, et al.
Improvement in fibromyalgia symptoms with acupuncture:
results of a randomized controlled trial.
Mayo Clin Proc. 2006;81(6):749–757Nelson DV, Bennett RM, Barkhuizen A, et al.
Neurotherapy of fibromyalgia?
Pain Med. 2010;11(6):912–919Cash E, Salmon P, Weissbecker I, et al.
Mindfulness meditation alleviates fibromyalgia symptoms
in women: results of a randomized clinical trial.
Ann Behav Med. 2015;49(3):319–330Hsu MC, Schubiner H, Lumley MA, et al.
Sustained pain reduction through affective self-awareness
in fibromyalgia: a randomized controlled trial.
J Gen Intern Med. 2010;25(10):1064–1070Astin JA, Berman BM, Bausell B, et al.
The efficacy of mindfulness meditation plus Qigong movement therapy
in the treatment of fibromyalgia: a randomized controlled trial.
J Rheumatol. 2003;30(10):2257–2262Menzies V, Lyon DE, Elswick RK, Jr, et al.
Effects of guided imagery on biobehavioral factors
in women with fibromyalgia.
J Behav Med. 2014;37(1):70–80Menzies V, Taylor AG, Bourguignon C.
Effects of guided imagery on outcomes of pain, functional status,
and self-efficacy in persons diagnosed with fibromyalgia.
J Altern Complement Med. 2006;12(1):23–30Liptan G, Mist S, Wright C, et al.
A pilot study of myofascial release therapy compared
to Swedish massage in fibromyalgia.
J Bodyw Mov Ther. 2013;17(3):365–370Jones KD, Sherman CA, Mist SD, et al.
A randomized controlled trial of 8-form Tai chi improves
symptoms and functional mobility in fibromyalgia patients.
Clin Rheumatol. 2012;31(8):1205–1214Wang C, Schmid CH, Rones R, et al.
A randomized trial of tai chi for fibromyalgia.
N Engl J Med. 2010;363(8):743–754Carson JW, Carson KM, Jones KD, et al.
A pilot randomized controlled trial of the Yoga of Awareness
program in the management of fibromyalgia.
Pain. 2010;151(2):530–539Cook AJ, Wellman RD, Cherkin DC, et al.
Randomized clinical trial assessing whether additional massage treatments
for chronic neck pain improve 12- and 26-week outcomes.
The spine journal : official journal of the North American Spine Society. 2015;15(10):2206–2215Field T, Diego M, Gonzalez G, et al.
Neck arthritis pain is reduced and range of motion
is increased by massage therapy.
Complement Ther Clin Pract. 2014;20(4):219–223Sherman KJ, Cherkin DC, Hawkes RJ, et al.
Randomized trial of therapeutic massage for chronic neck pain.
Clin J Pain. 2009;25(3):233–238Sherman KJ, Cook AJ, Wellman RD, et al.
Five-week outcomes from a dosing trial of therapeutic
massage for chronic neck pain.
Ann Fam Med. 2014;12(2):112–120Evans R, Bronfort G, Schulz C, et al.
Supervised Exercise With And Without Spinal Manipulation
Performs Similarly And Better Than Home Exercise
For Chronic Neck Pain: A Randomized Controlled Trial
Spine (Phila Pa 1976). 2012 (May 15); 37 (11): 903–914Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Yu F, Adams AH.
A Randomized Trial of Chiropractic Manipulation and Mobilization
for Patients With Neck Pain: Clinical Outcomes From
the UCLA Neck-Pain Study
Am J Public Health 2002 (Oct); 92 (10): 1634–1641Maiers M, Bronfort G, Evans R, Hartvigsen J, Svendsen K, Bracha Y, et al.
Spinal Manipulative Therapy and Exercise For Seniors
with Chronic Neck Pain
Spine J. 2014 (Sep 1); 14 (9): 1879–1889Gudavalli MR, Salsbury SA, Vining RD, et al.
Development of an attention-touch control for manual cervical distraction:
a pilot randomized clinical trial for patients with neck pain.
Trials. 2015:16259Berman BM, Lao L, Langenberg P, et al.
Effectiveness of acupuncture as adjunctive therapy in
osteoarthritis of the knee: a randomized, controlled trial.
Ann Intern Med. 2004;141(12):901–910Berman BM, Singh BB, Lao L, et al.
A randomized trial of acupuncture as an adjunctive therapy
in osteoarthritis of the knee.
Rheumatology (Oxford) 1999;38(4):346–354Chen LX, Mao JJ, Fernandes S, et al.
Integrating acupuncture with exercise-based physical therapy
for knee osteoarthritis: a randomized controlled trial.
J Clin Rheumatol. 2013;19(6):308–316Suarez-Almazor ME, Looney C, Liu Y, et al.
A randomized controlled trial of acupuncture for osteoarthritis
of the knee: effects of patient-provider communication.
Arthritis Care Res (Hoboken) 2010;62(9):1229–1236Clegg DO, Reda DJ, Harris CL, et al.
Glucosamine, chondroitin sulfate, and the two in combination
for painful knee osteoarthritis.
N Engl J Med. 2006;354(8):795–808Frestedt JL, Walsh M, Kuskowski MA, et al.
A natural mineral supplement provides relief from
knee osteoarthritis symptoms: a randomized
controlled pilot trial.
Nutr J. 2008:79Leffler CT, Philippi AF, Leffler SG, et al.
Glucosamine, chondroitin, and manganese ascorbate for
degenerative joint disease of the knee or low back:
a randomized, double-blind, placebo-controlled pilot study.
Mil Med. 1999;164(2):85–91McAlindon T, Formica M, LaValley M, et al.
Effectiveness of glucosamine for symptoms of knee osteoarthritis:
results from an internet-based randomized double-blind controlled trial.
Am J Med. 2004;117(9):643–649Messier SP, Mihalko S, Loeser RF, et al.
Glucosamine/chondroitin combined with exercise for the
treatment of knee osteoarthritis: a preliminary study.
Osteoarthritis Cartilage. 2007;15(11):1256–1266Rindone JP, Hiller D, Collacott E, et al.
Randomized, controlled trial of glucosamine for
treating osteoarthritis of the knee.
West J Med. 2000;172(2):91–94Rubin BR, Talent JM, Kongtawelert P, et al.
Oral polymeric N-acetyl-D-glucosamine and osteoarthritis.
J Am Osteopath Assoc. 2001;101(6):339–344Zenk JLHT, Kuskowski MA.
The effects of milk protein concentrate on the symptoms of
osteoarthritis in adults: an exploratory, randomized,
double-blind, placebo-controlled trial.
Current Therapeutic Research. 2002;63(7):430–442.Perlman AI, Ali A, Njike VY, et al.
Massage therapy for osteoarthritis of the knee:
a randomized dose-finding trial.
PLoS One. 2012;7(2):e30248Perlman AI, Sabina A, Williams AL, et al.
Massage therapy for osteoarthritis of the knee:
a randomized controlled trial.
Arch Intern Med. 2006;166(22):2533–2538Altman R, Asch E, Bloch D, et al.
Development of criteria for the classification and reporting of
osteoarthritis. Classification of osteoarthritis of the knee.
Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association.
Arthritis Rheum. 1986;29(8):1039–1049Kim LS, Axelrod LJ, Howard P, et al.
Efficacy of methylsulfonylmethane (MSM) in osteoarthritis pain
of the knee: a pilot clinical trial.
Osteoarthritis Cartilage. 2006;14(3):286–294Najm WI, Reinsch S, Hoehler F, et al.
S-adenosyl methionine (SAMe) versus celecoxib for the treatment
of osteoarthritis symptoms: a double-blind cross-over trial.
[ISRCTN36233495]
BMC Musculoskelet Disord. 2004:56Brismee JM, Paige RL, Chyu MC, et al.
Group and home-based tai chi in elderly subjects with
knee osteoarthritis: a randomized controlled trial.
Clin Rehabil. 2007;21(2):99–111Hartman CA, Manos TM, Winter C, et al.
Effects of T’ai Chi training on function and quality of life
indicators in older adults with osteoarthritis.
J Am Geriatr Soc. 2000;48(12):1553–1559Tsai PF, Chang JY, Beck C, et al.
A pilot cluster-randomized trial of a 20-week Tai Chi program
in elders with cognitive impairment and osteoarthritic knee:
effects on pain and other health outcomes.
J Pain Symptom Manage. 2013;45(4):660–669Wang C, Schmid CH, Hibberd PL, et al.
Tai Chi is effective in treating knee osteoarthritis:
a randomized controlled trial.
Arthritis Rheum. 2009;61(11):1545–1553Park J, McCaffrey R, Dunn D, et al.
Managing osteoarthritis: comparisons of chair yoga, Reiki,
and education (pilot study)
Holist Nurs Pract. 2011;25(6):316–326The International Classification of Headache Disorders.
Cephalalgia. (2) 2004;24(Suppl):19–160The International Classification of Headache Disorders,
3rd edition (beta version)
Cephalalgia. 2013;33(9):629–808Coeytaux RR, Kaufman JS, Kaptchuk TJ, et al.
A randomized, controlled trial of acupuncture for chronic daily headache.
Headache. 2005;45(9):1113–1123Moraska AF, Stenerson L, Butryn N, et al.
Myofascial trigger point-focused head and neck massage for recurrent
tension-type headache: a randomized, placebo-controlled clinical trial.
Clin J Pain. 2015;31(2):159–168Harel Z, Gascon G, Riggs S, et al.
Supplementation with omega-3 polyunsaturated fatty acids in the
management of recurrent migraines in adolescents.
J Adolesc Health. 2002;31(2):154–161Ramsden CE, Faurot KR, Zamora D, et al.
Targeted alteration of dietary n-3 and n-6 fatty acids for the
treatment of chronic headaches: a randomized trial.
Pain. 2013;154(11):2441–2451Blanchard EB, Appelbaum KA, Nicholson NL, et al.
A controlled evaluation of the addition of cognitive therapy to
a home-based biofeedback and relaxation
treatment of vascular headache.
Headache. 1990;30(6):371–376Devineni T, Blanchard EB.
A randomized controlled trial of an internet-based treatment
for chronic headache.
Behav Res Ther. 2005;43(3):277–292D’Souza PJ, Lumley MA, Kraft CA, et al.
Relaxation training and written emotional disclosure for
tension or migraine headaches: a randomized, controlled trial.
Ann Behav Med. 2008;36(1):21–32Holroyd KA, O’Donnell FJ, Stensland M, et al.
Management of chronic tension-type headache with tricyclic antidepressant
medication, stress management therapy, and their combination:
a randomized controlled trial.
JAMA. 2001;285(17):2208–2215Scharff L, Marcus DA, Masek BJ.
A controlled study of minimal-contact thermal
biofeedback treatment in children with migraine.
J Pediatr Psychol. 2002;27(2):109–119Slavin-Spenny O, Lumley MA, Thakur ER, et al.
Effects of anger awareness and expression training versus
relaxation training on headaches: a randomized trial.
Ann Behav Med. 2013;46(2):181–192Haas M, Spegman A et al. (2010)
Dose Response and Efficacy of Spinal Manipulation for Chronic
Cervicogenic Headache: A Pilot Randomized Controlled Trial
Spine J. 2010 (Feb); 10 (2): 117–128Boline, PD, Kassak, K, Bronfort, G, Nelson, C, and Anderson, AV.
Spinal Manipulation vs. Amitriptyline for the Treatment of Chronic
Tension-type Headaches: A Randomized Clinical Trial
J Manipulative Physiol Ther 1995 (Mar); 18 (3): 148–154Hoyt WH, Shaffer F, Bard DA, et al.
Osteopathic manipulation in the treatment of muscle-contraction headache.
J Am Osteopath Assoc. 1979;78(5):322–325Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV:
The Efficacy of Spinal Manipulation, Amitriptyline and the Combination
of Both Therapies for the Prophylaxis of Migraine Headache
J Manipulative Physiol Ther 1998 (Oct); 21 (8): 511–519Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al.
Noninvasive Treatments for Low Back Pain
Comparative Effectiveness Review no. 169
Agency for Healthcare Research and Quality; (February 2016)Deare JC, Zheng Z, Xue CC, et al.
Acupuncture for treating fibromyalgia.
The Cochrane database of systematic reviews. 2013:5Cd007070Manheimer E, Cheng K, Linde K, et al.
Acupuncture for peripheral joint osteoarthritis.
The Cochrane database of systematic reviews. 2010;(1):Cd001977Posadzki P, Ernst E.
Spinal manipulations for the treatment of migraine:
a systematic review of randomized clinical trials.
Cephalalgia. 2011;31(8):964–970Haaz S, Bartlett SJ.
Yoga for arthritis: a scoping review.
Rheum Dis Clin North Am. 2011;37(1):33–46Sharma M.
Yoga as an alternative and complementary approach for arthritis:
a systematic review.
J Evid Based Complementary Altern Med. 2014;19(1):51–8Franke H, Franke JD, Fryer G.
Osteopathic manipulative treatment for nonspecific low back pain:
a systematic review and meta-analysis.
BMC Musculoskelet Disord. 2014;15:286Wu D, Huang Y, Gu Y, et al.
Efficacies of different preparations of glucosamine for the treatment
of osteoarthritis: a meta-analysis of randomised,
double-blind, placebo-controlled trials.
Int J Clin Pract. 2013;67(6):585–594Rubinstein SM, Terwee CB, Assendelft WJ, de Boer MR, van Tulder MW.
Spinal manipulative therapy for acute low back pain:
an update of the cochrane review.
Spine (Phila Pa 1976) 2013;38(3):E158–77
Return to ALT-MED/CAM ABSTRACTS
Return to SPINAL PAIN MANAGEMENT
Since 5-24-2018
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |