

The Nordic Maintenance Care Program: Maintenance Care Reduces
the Number of Days With Pain in Acute Episodes and Increases
the Length of Pain Free Periods for Dysfunctional Patients
With Recurrent and Persistent Low Back Pain -
A Secondary Analysis of a Pragmatic
Randomized Controlled TialThis section was compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Chiropractic & Manual Therapies 2020 (Apr 21); 28: 19 ~ FULL TEXT
OPEN ACCESS Andreas Eklund, Jan Hagberg, Irene Jensen, Charlotte Leboeuf-Yde, Alice Kongsted, Peter Lövgren, Mattias Jonsson, Jakob Petersen-Klingberg, Christian Calvert & Iben Axén
Karolinska Institutet,
Institute of Environmental Medicine,
Unit of Intervention and Implementation Research for Worker Health,
Stockholm, Sweden.
BACKGROUND: A recent study showed that chiropractic patients had fewer days with bothersome (activity-limiting) low back pain (LBP) when receiving care at regular pre-planned intervals regardless of symptoms (‘maintenance care’, MC) compared to receiving treatment only with a new episode of LBP. Benefit varied across psychological subgroups. The aims of this study were to investigate 1) pain trajectories around treatments, 2) recurrence of new episodes of LBP, and 3) length of consecutive pain-free periods and total number of pain-free weeks, for all study participants as well as for each psychological subgroup.
METHODS: A secondary analysis of data from a randomized controlled trial of patients (n = 319) seeking chiropractic care for recurrent or persistent LBP used 52 weekly estimates of days with bothersome (activity-limiting) LBP. First, a generalized estimating equations analysis was used to compare the pain trajectory before and after the initial treatment in every new treatment period. Thereafter, a time-to-event analysis (using Cox regression) estimated time to/risk of a new LBP episode. The analyses were performed on i) all study participants and ii) separately for each psychological sub-group (named adaptive copers, interpersonally distressed and dysfunctional) classified by the West Haven-Yale Multidimensional Pain Inventory.
RESULTS: Patients receiving MC had flat pain trajectories around each new treatment period and reported fewer days with pain compared to patients receiving the control intervention. The entire effect was attributed to the dysfunctional subgroup who reported fewer days with activity limiting pain within each new LBP episode as well as longer total pain-free periods between episodes with a difference of 9.8 weeks (CI 95% 3.3, 16.3) compared to the control group. There were no differences in the time to/risk of a new episode of LBP in either of the subgroups.
There are more articles like this @ our:
MAINTENANCE CARE PageCONCLUSIONS: Data support the use of MC in a stratified care model targeting dysfunctional patients for MC. For a carefully selected group of patients with recurrent and persistent LBP the clinical course becomes more stable and the number of pain-free weeks between episodes increases when receiving MC. Understanding how subgroups of patients are likely to be affected by MC may help align patients’ and clinicians’ expectations based on realistic outcomes.
TRIAL REGISTRATION Clinical trials.gov; NCT01539863
From the Full-Text Article:
Background
Low back pain (LBP) is a recurrent and persistent non-communicable condition ranked highest in in the world in terms of disability and resulting in a major societal burden. [1, 2] Secondary or tertiary preventive strategies are needed to manage a global health challenge such as LBP. A modest number of interventions have been shown to be effective in managing and treating recurrent and persistent LBP. [3] However, only exercise and exercise combined with education have been shown to reduce the number of new episodes. [4–7]
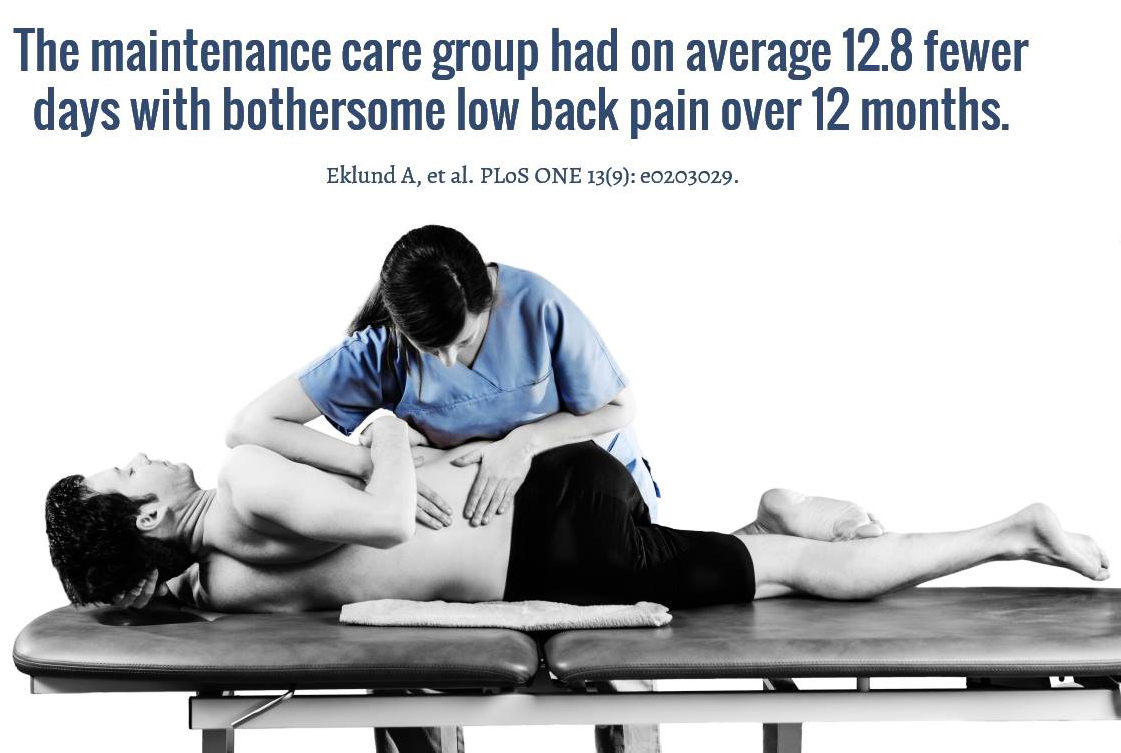
Manual treatments performed by chiropractors have been found to be effective in reducing pain intensity and disability for patients with LBP and are recommended in current practice guidelines. [8, 9] About 98% of all chiropractors who are members of the Swedish Chiropractic Association consider a treatment strategy known as maintenance care (MC) to be clinically useful and beneficial for patients with recurrent and persistent musculoskeletal pain. [10] MC is a secondary/tertiary treatment strategy where patients are treated at regular intervals over a lengthy period of time with the aim of preventing future episodes (secondary prevention) or managing persistent pain (tertiary prevention). [11, 12] In a joint initiative, researchers in Sweden, Denmark and Finland have investigated the frequency, indications and content of MC. [13–21] Based on their findings a multicenter pragmatic randomized clinical trial was conducted in Sweden from 2012 to 2016. [22, 23] The trial found that MC was effective in reducing the total number of days with activity limiting (bothersome)LBP during a 12 month period compared to treatment ‘when needed’. [23] In total the MC group (n = 163) reported 12.8 (95% CI: 10.1, 15.5) fewer days with activity limiting LBP compared to the control group (n = 158) and received 1.7 (95% CI: 1.8, 2.1) more treatments.
In a secondary analysis of the data from the RCT it was found that psychological sub-groups defined by the Swedish version of the West Haven-Yale Multidimensional Pain Inventory (MPI-S) could identify responders and non-responders to MC. [24]
The MPI-S is a comprehensive patient-reported screening instrument based on the cognitive behavioral model which was developed to capture and measure the experience of chronic pain. [25] The Swedish version of the instrument has 34 items that can be used to classify patients into three clinically relevant and valid subgroups: adaptive copers, interpersonally distressed and dysfunctional. [26–29] Adaptive copers (AC) are characterized by low pain severity, low interference with everyday life, low life distress, a high activity level and a high perception of life control. Interpersonally distressed (ID) tend to perceive negative responses by spouses or significant others to their pain behavior and complaints, for example not being supportive/helpful, and expressing irritation, frustration and anger. Dysfunctional (DYS) individuals are characterized by high pain severity, marked interference with everyday life, high affective distress, low perception of life control and low activity levels.
Patients who were classified as dysfunctional reported statistically and clinically significantly fewer days with bothersome (activity-limiting) LBP (– 30.0; 95% CI: – 36.6, – 23.4) in the MC group compared to the control group. On the other hand, patients who were classified as adaptive coper reported a worse outcome where the number of days with bothersome (activity-limiting) LBP was higher (10.7; 95% CI 4.0, 17.5) in the MC groups even though they received a greater number of treatments (3.9; 95% CI: 3.5, 4.2) compared to the control group. There is now compelling evidence that stress the importance of careful the selection of patients for MC to include those who have recurrent or persistent low back pain, a dysfunctional psychological profile and a good initial response to manual therapy.
It is imperative that we undertake research and implement preventive strategies with clear and precise definitions of target populations and disease states. The definition of new episodes for a recurrent disorder such as LBP requires a clear definition of ‘recovery’. De Vet et al. suggested that an episode of LBP should be defined as at least 24 h of pain with at least four pain-free weeks before and after. [30] The prevalence of four consecutive pain-free weeks has been studied in a number of populations and found to represent a good marker of non-episodes. [31–33] In addition, there is a logical inverse dose-response relationship between consecutive numbers of pain-free weeks and previous duration of pain. [31] Thus, a period of four pain-free weeks can be used as a marker of recovery, necessary when defining an episodes. []
The optimal dose of treatments for the long-term management of recurrent and persistent LBP has not been established. In fact, we are not sure whether the effect of MC is a matter of dose (a higher number of visits yielding a reduction of pain irrespective of when the visits occur) or timing (preventing the number of episodes or reducing the number of days within each episode by timing the treatment before or in the early stage of the new event). If the effect of MC is related to the timing of visits, patients who consult at different stages in their long-term pain trajectory and pain around the treatments would have different outcome profiles (i.e. MC treatments should take place before the recurrence of pain and control treatments after the recurrence of pain). The previous secondary analysis of these data, which considered outcome in relation to psychological sub-groups [24], suggested that the outcome is not dependent on number of treatments because the effect of MC seen in the dysfunctional subgroup was achieved with the same number of visits as in the control group. Indeed, a larger number of MC visits could potentially be harmful for some patients, given the outcome for the adaptive coper subgroup. To further our understanding of how MC affects LBP, another secondary analysis of the data from the RCT was performed to investigate the trajectory of pain episodes, the occurrence of (time to/risk of) new episodes of LBP and pain-free periods in relation to patients receiving care when experiencing a symptomatic relapse.
Method
Aim The overall aim of this project was to explore how MC affects the bothersome (activity-limiting) LBP around treatment periods, new episodes of LBP and pain-free periods between episodes as compared to patients receiving care when experiencing a symptomatic relapse. The specific objectives were to compare the following for i) all participants in the trial as well as the ii) psychological subgroups defined by the MPI-S instrument:
The pain trajectory before and after a single visit or the first visit in every new treatment period.
The time to and risk of a new episode following the first recovery period.
The length of consecutive pain-free periods and total number of pain-free weeks during the study period.
Design
This study is a secondary analysis of data from a pragmatic, multicenter, investigator- and assessor- blinded randomized controlled trial with a two-arm parallel design. [22–24] The trial was based on the findings of the Nordic Maintenance Care program and made use of all the current evidence in the field [13–21]. The primary aim of the trial was to measure the differences in outcome of MC on patients with recurrent or persistent LBP. A total of 35 licensed chiropractors from the Swedish Chiropractic Association requited patients in a nationwide practice-based research-network. The follow-up period was 52 weeks and the primary outcome of the trial was “number of days with bothersome (activity-limiting) LBP” measured using weekly text-messages, SMS. The trial design has been extensively reported in a published protocol paper [22] and in two previous papers evaluating the outcomes of MC. [23, 24]
Participants

Table 1 Patients with recurrent and persistent LBP, who had responded favorably to an initial course of chiropractic care, were recruited in a consecutive sequence between 2012 and 2016 from chiropractic clinics that were part of a nationwide practice-based research network in Sweden. Patients were screened in a three-stage procedure, i.e. at the first visit (baseline 1), the fourth visit (baseline 2), and at study start (baseline 3). See Table 1 for the inclusion criteria at each stage of the trial. Both clinicians and patients received follow-up questionnaires at 12 months. During the inclusion procedure (baseline 1, 2, and 3) patients followed a normal treatment pathway and were included in the trial (i.e. randomly allocated to one of the treatment arms), when the clinician would, as in clinical practice, either schedule the patient for MC or end the current treatment plan.
One of the key components and inclusion criterion of the trial was to select patients who reported clinical benefit from chiropractic care during the initial treatment. Initial clinical benefit was assessed at the 4th visit using the global perceived improvement scale (single question with one answer in 5 levels: definitely worse, probably worse, unchanged, probably improved, definitely improved). If the patients stated that they were “definitely improved” by the fourth visit, initial clinical benefit was considered evident. Previous research has shown that using the global perceived improvement scale in this way can predict a favourable long-term outcome from chiropractic care at 3, 6, and 12 months. [34–37] According to research from the Nordic Maintenance Care program, early favorable treatment response is an indication for recommending MC and this step was therefore a core component of the design to reinforce the pragmatic nature of the trial. [10, 16–18, 20, 21]
Once patients were screened at the 3 baseline steps and considered candidates for the study, they were invited to partake in the study and asked to sign an informed consent form with information about the trial. It was also made clear to patients in the written information that they were free to withdraw from the project at any point without detriment to their relationship with the clinician.
Interventions
The two arms of the trial have been described as MC (preventive treatment, i.e. clinician-controlled) and control (symptom-guided treatment, i.e. patient controlled). The MC group received regularly scheduled treatments, 1–3 months apart during the 52 weeks of follow-up. If the patient had a relapse of pain, a more intense period of visits was scheduled until the patient once again was suitable for a MC plan. The control group was instructed to seek care only if they experienced a symptomatic relapse. In such cases a period of frequent visits would be scheduled until maximum benefit was reached, after which the patients were again instructed to seek care if the LBP reoccurred. Content of care within the two treatment arms were similar, consisting of spinal manipulation, information/advice and soft tissue treatment, as was the level of attention given to the patients. [23] Both groups had 50% of the treatment fee subsidized by the participating clinicians. Prior to the start of the trial, clinicians were given a carefully written study protocol with instructions about the trial procedures. Much effort, by means of physical meetings and telephone contact, was made to ensure that all clinicians had understood and would comply with the study procedures.
Randomization and information to participants
A statistician at Karolinska Institutet generated 40 permuted blocks of 10 participants with a 1:1 allocation ratio according to a randomization schedule. Each clinician received 10 opaque, sealed envelopes containing information about the procedure the patient had been randomly allocated to. The envelopes were opened in front of the patient at the initial visit of the study. Clinicians were instructed to inform patients that 1) the two treatment arms were different procedures currently being used in practice, and 2) there was no evidence to suggest that one strategy was more effective than the other. [22]
Outcome variables
The primary outcome of the trial was number of days with bothersome (activity-limiting) LBP. It was recorded weekly using an automated text message system (SMS-track®) [38–40] that allowed the researchers to monitor the data collection process from a web-interface in real-time. Thus, patients received the message: “On how many days during the past week were you bothered by your lower back (i.e. it affected your daily activities or routines)? Please answer with a number between 0 and 7”. If the patient failed to respond to the weekly SMS, an automatic reminder was sent after 48 h. If the patient failed to respond after 2 weeks, a research assistant called the patient to answer any concerns that may have caused the patient not to respond.
At follow-up the chiropractor filled in a questionnaire where they were asked to review each patient’s clinical record and document the dates of all visits during the study period. This information was then used to model the trajectory analysis.
To apply the definition by de Vet et al. [30] as closely as possible to our data, a pain-free week was classified as a week with ≤1 day with activity-limiting LBP in the time-to-event analysis. The classification of pain-free weeks as “≤2 days with bothersome (activity-limiting) LBP” instead of “<2 days with bothersome (activity-limiting) LBP” minimized the risk of misclassification of weeks with temporary short (< 24 h) exacerbations of LBP as episodes. Thus, a new pain episode was defined as a week with ≥2 [2–7] days of bothersome (activity-limiting) LBP preceded by ≥4 consecutive pain-free weeks according to the suggested classification above. A pain episode was considered ongoing until ≥4 consecutive pain-free weeks were recorded.
A treatment-period was defined as a single visit or as the first of a series of visits with an interval of ≤2 weeks apart, followed by ≥3 consecutive weeks without any visits to the chiropractor (1 month between visits). MC visits were scheduled 1–3 months apart according to the normal procedures used in clinical practice [41] as reported in the study protocol [22]. The definition of treatment period was chosen to include each MC visit as a new period, any interval between treatments of less than 1 month was considered an active treatment period. [41] In the analysis, each study participant contributed with all treatment periods during the 52–week study period.
A pain-trajectory was defined as “the number of days with bothersome (activity-limiting) LBP per week, during a 7–week period around the week of a single visit or the first visit in a new treatment period” (3 weeks before and 3 weeks after the treatment). The trajectory (mean number of days with pain) for each of the 7 weeks for all single visits or new treatments periods for per group was estimated.
Psychological sub-groups
The MPI-S subgroups have been extensively described in the previous publication, which reported the sub-group evaluation of effect of MC. [24] Patients were classified by the MPI-S instrument, as part of the first visit screening procedure (baseline 1).
Statistical methods
The data from the RCT was analyzed with an intention to treat analysis. Estimates in this study were reported with arithmetic means and 95% confidence intervals. Only individuals who had > 12 weeks of complete SMS data and follow up data for number and dates of visits were included in the analyses.
Data relating to the first objective were analyzed in a longitudinal model which looked at the pain trajectory around the initial visit of each treatment period. Mean number of days with bothersome (activity-limiting) LBP was calculated for each group and for each week during the 7–week treatment period (3 weeks before the visit, week of the visit and 3 weeks after). If two visits were separated by 3 weeks without visits (i.e. defined as two separate treatment periods in the statistical model), the analysis would then double count the last 3 weeks [5–7] in the first treatment period and the first 3 weeks [1–3] in the following treatment period. The mean number of visits for the whole cohort over 12 months was six visits, so the probability of double counting weeks without pain (as described above) was considered low, with little risk of distorting the results. Data were analyzed by means of a Generalized Estimating Equations (GEE) linear regression model, using an appropriate correlation structure (the best ‘quasi-likelihood under the independence model criterion (QIC)’ value for each strata) and a robust estimator of variance (robust to non-constant error variance).
The analysis included treatment group and time (both as study period (52 weeks) and treatment period (7 weeks)) as continuous variables. These covariates were tested as single variables in combinations as well as interaction terms. Co-variates were excluded based on test of model effects, and all variables with a significance level of p < 0.20 were considered for the regression model. The best model structure was further decided based on goodness of fit values (QIC-value). All remaining variables in the final models, chosen based on the best goodness of fit, ended up with significance levels of p < 0.05. Data were also analyzed using a Mixed Model framework. The results of the two procedures were very similar; GEE was chosen rather than the mixed model framework because of its ease of use. Results were presented in graphs, with lines representing mean values and estimated group differences for each week of days with bothersome pain, illustrating pain trajectories for the control and intervention groups.
Data relating to the second objective of this study were analyzed in a time-to-first event model using Cox regression in a survival analysis, estimating the Hazard Ratio of experiencing new LBP episodes. Only individuals who initially reached a recovered state (≥4 consecutive weeks free from bothersome LBP), were included in the Cox regression.
In the third objective, differences between groups for i) time-to-event and ii) length of consecutive pain-free periods and total number of pain-free weeks were tested using ANOVA.
Data were analyzed for all participants (included in the primary analysis [23]), in line with the intention to treat analysis as well as stratified according to the 3 MPI-S subgroups (adaptive copers, interpersonally distressed and dysfunctional included in the subgroup analysis [24]).
Results
Table 2

Figure 1

Figure 2
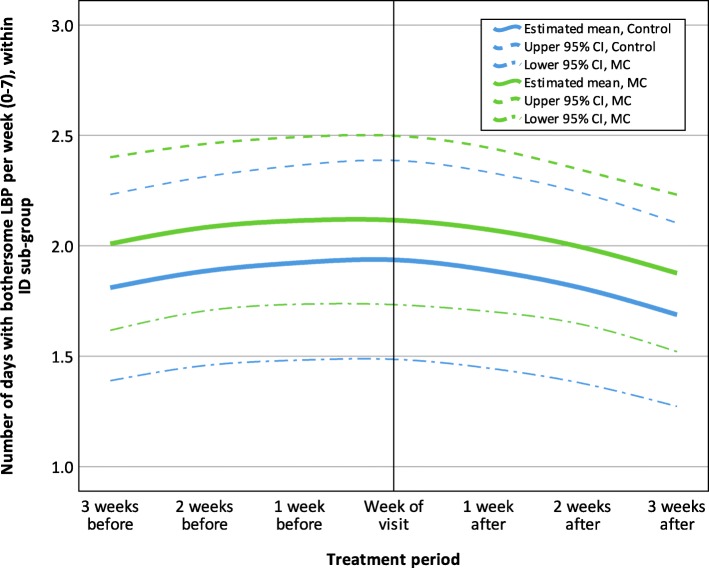
Figure 3

Figure 4
Table 3

Figure 5
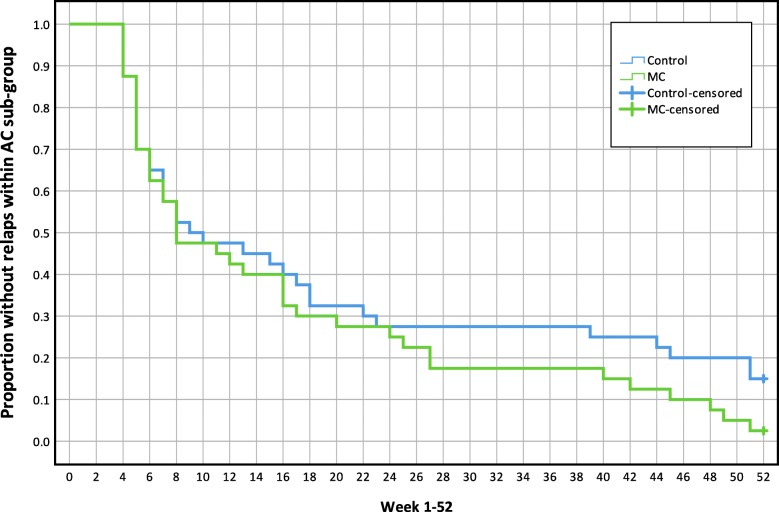
Figure 6

Figure 7
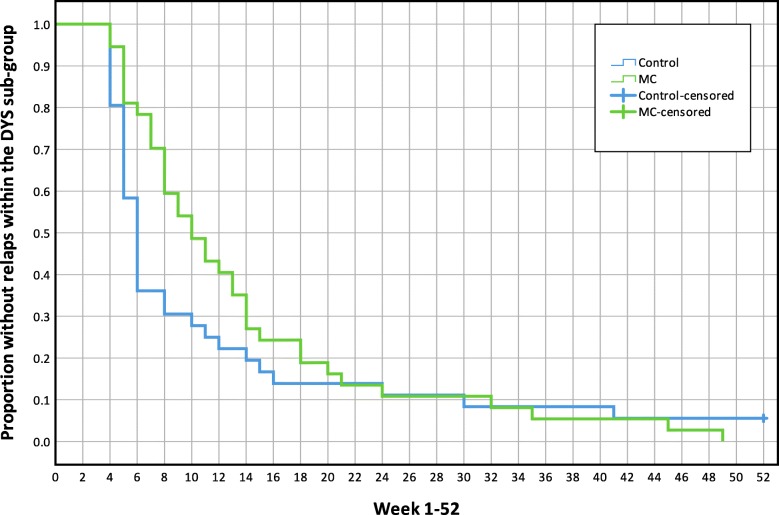
Figure 8 As previously reported, 321 participants were randomly allocated into the two study groups after the initial inclusion procedure. [23] During the study period, 16,692 SMS messages were sent with a response rate of 98.9%. Two participants had ≥12 weeks of missing SMS data and were excluded from the dataset, leaving 319 individuals to be included in the analysis. [23]
Two hundred and fifty-four participants had at least one treatment and could be included in the longitudinal pain trajectory analysis. A total of 1103 treatment-period sequences were identified during the 12–month study period (344 control, 759 MC) and were used for the analyses. In all, 250 participants reached at least one recovered state and could be included in the time-to-first-event analysis.
The trajectory analysis captured a sample with fewer females than the samples in the total and the survival analyses. There were also somewhat fewer individuals classified as adaptive copers in the control group for the trajectory analysis than for the total and the survival analyses. Other than these differences the samples across analysis groups and across treatment groups were similar. Descriptive data for the participants included in each analysis are reported in Table 2.
Pain trajectory analysis before and after a single visit
or the first visit in every new treatment period
The pain trajectories around the visits were different for the two treatment groups, when all participants were included. The control group showed a steeper increase of pain during the weeks prior to the visit and reached the highest number of days with pain in the week of treatment, when the largest mean difference between groups can be seen (0.46 bothersome (activity-limiting) days with LBP per week; 95% CI =0.16, 0.76). The MC group had a less dramatic trajectory, reporting fewer days with bothersome (activity-limiting) LBP compared to the control group. The pain trajectory for all participants is reported in Figure 1.
In the adaptive coper and interpersonally distressed subgroups the estimates across the seven measurements were similar, with no apparent difference between the control and MC groups with regards to their LBP trajectories. The trajectories for adaptive coper and interpersonally distressed subgroups are shown in Figures 2 and 3.
The LBP trajectory for the dysfunctional subgroup demonstrates great differences between treatment groups throughout the treatment period, with the largest mean difference around the visit (0.86; 95% CI = 0.39, 1.32). Like the analysis with all participants, the control group had a steep increase in LBP up to the week of the treatment and a decreasing trend after the visit; in comparison the MC group had a flat trajectory. The LBP trajectory for the dysfunctional subgroup is reported in Figure 4.
In Supplementary Material 1, weekly adjusted mean group differences of days with LBP for the treatment periods for the whole group and all MPI-S subgroups are reported.
The time to and risk of a new episode following the first recovery period There were no mean differences between treatment groups in the Hazard Ratio of new episodes or time-to-event in any of the analyses (all participants or MPI-S subgroups). Results are reported in Table 3. Kaplan-Maier graphs illustrate survival functions for each analysis in Figures. 5, 6, 7 and 8.
The length of consecutive pain-free periods and total number
of pain-free weeks during the study period
There were no differences between treatment groups in the mean length of pain-free periods or in the mean total number of pain-free weeks when all participants were included in the analysis. When the data were stratified according to the MPI-S subgroups, MC resulted in 9.8 (CI95% 3.3, 16.3) more pain-free weeks (mean) compared to control in the dysfunctional sub-group during the 12–month study period. In the adaptive coper and interpersonally distressed sub-groups the mean differences were small and uncertain (AC –1.9, 95% CI: – 8.7, 4.9; ID 1.0, 95% CI: – 13.2, 15.3). The results are reported in Table 3.
Discussion
This study is the first to investigate how patients benefit from MC using an in-depth analysis of the clinical course of LBP. It answers questions about how MC affects the number of days with bothersome (activity-limiting) LBP over time by exploring the trajectory around the visit to the chiropractor, the time to and risk of new episodes, and length of pain-free periods (consecutive and total number of).
We found that patients receiving MC had flat LBP trajectories around each new treatment period, as their appointments were unrelated to their symptoms, as opposed to the control group, who were encouraged to call in ‘when needed’. The MC group also had fewer days of bothersome (activity-limiting) LBP than patients receiving the control intervention, who demonstrated more acute episodes.
However, in the adaptive coper and interpersonally distressed groups there were no differences for any of the reported outcomes and the entire difference between MC and control groups was attributed to the dysfunctional subgroup. In the dysfunctional subgroup, there were no differences in the time to/risk of first new episode although MC patients reported more pain-free weeks than the control group. In other words, the clinical course was stabilized by reducing the number of days with LBP per week of each new episode and by increasing the total number of pain-free weeks in the dysfunctional group. As the number of days with bothersome LBP has been shown to correlate with pain intensity [42], it is likely that these patients not only experienced fewer days with LBP but also less intense pain when in remission. These findings are of clinical relevance and may directly affect the delivery of MC in chiropractic practice so that appropriate patients (those with a dysfunctional profile) should be offered MC instead of indiscriminately recommending the procedure to all patients which seems to be the case currently.
The use of weekly SMS with exceptionally few missing data points allows for a detailed analysis of the LBP trajectories with a low risk of recall bias. Therefore, the data used in this trial can be considered robust and of high quality. The inclusion procedure and execution of the MC protocol have been carefully designed to incorporate all the available evidence in the field and to mimic the procedure used in clinical practice as closely as possible. The multi-center pragmatic design with clinics distributed across the country and a high number of involved clinicians allows us to generalize the results to normal clinical practice within the Nordic countries. Although it has been used previously in several trials, measuring the number of days with bothersome (activity-limiting) LBP is novel. A limitation with regards to the clinical relevance of the findings is the lack of knowledge of the exact properties of the primary outcome (number of days with bothersome, activity-limiting, LBP) concerning how it correlates with other health measurements (other than pain intensity). However, the benefit of the measurement is that it reports only the kind of pain that is relevant to the patient. Another potential concern is the way we have classified LBP episodes in this study, which may result in a risk of systematic error that could have underestimated the length and prevalence of LBP episodes. It is known that LBP has a highly individual trajectory and often fluctuates over time rather than being constantly present. [43, 44] We defined our LBP episodes as at least 2 days with pain per week. Presently, no validated definition of a painful event seems to exist; i.e. it is not known for how long pain must be present to be considered a problem by the individual suffering the pain. We defined an event of pain as at least 2 days during a week, assuming that this would represent a problem that was noticeable and relevant.
This study demonstrated that, among dysfunctional patients, MC reduced the number of days of activity limiting LBP in each new episode and people enjoyed more pain-free weeks. At most, the mean difference among dysfunctional patients was 0.86 (CI95%: 0.39, 1.32) fewer days with pain in each new episode while also enjoying 9.8 (3.3, 16.3) more pain free weeks, resulting in a total of 30.0 (95% CI: 36.6, 23.4) fewer days with pain for the entire 52 week period. [24] These estimates are likely to be clinically relevant for the individual and probably cost effective from a societal perspective given that the mean number of visits between MC and control was equal. [24] However, we do not understand the mechanism of this effect. MC may, for example, have a biomechanical effect on joints/tissues by maintaining function and reducing pain sensitivity, but then this should be observed also in the other subgroups of patients. This was not the case and – in fact – one group should not receive MC as it worsened their situation. [24] It is therefore more likely that MC has a psychological effect in the group that has worst coping strategies and struggle to manage their pain, whereby meeting and interacting with the clinician reduces the severity of the pain experience. The explanation could also be behavioral, whereby pre-scheduled appointments help people to act more appropriately, i.e. adhere to exercise programs, challenge fearful beliefs and keep active despite pain etc. However, why this would work only for the dysfunctional group is unclear.
Irrespective of the mechanism is seems that the effectiveness of MC among dysfunctional patients could depends on the timing of visits to the chiropractor, i.e. independent of pain ideally before or early in a new episode. If this is an important part of the mechanism, patients with regular LBP episodes could be more successfully scheduled according to a structured MC program because of improved precision in the timing of treatments due to predictability of the pain trajectory. If this rationale holds true these patients may benefit most from the intervention through a reduction of the impact of the most severe periods of pain, perhaps reducing the risk of sick leave, presenteeism and limitations on the activities of daily living.
However, at this point in time the mechanisms behind MC are unknown and remain a question for future projects. Future research should therefore focus on replicating the findings from this trial and understanding why MC has a positive effect on dysfunctional patients but appears to have the opposite effect for adaptive copers. A suitable approach would be to conduct an RCT on dysfunctional patients, randomizing them to a chiropractic maintenance care program or a program consisting of psychological support, advice and reassurance to tease out if it is mainly the physical component of the treatment that ‘works’ or if it is the psychological component that is responsible for this outstanding result. Another important avenue for future research relates to health economic evaluations of MC to better understand and model the societal consequences of MC. To establish if the procedure is cost-effective is imperative for policy makers and health care funders and a key component when implementing the procedure on a large scale.
The message for the patient should be that MC is not a cure that prevents new episodes but rather a management strategy that may reduce bothersome (activity-limiting) LBP over time for a carefully selected group of patients with a dysfunctional profile. Patents who adapt well to their pain, who experience only little interference, have an active lifestyle and do not experience high levels of distress are not suited for MC and should be cared for on an episode to episode basis. Such a message could potentially align expectations to realistic outcomes and may result in a higher degree of trust and a more effective therapeutic alliance between the clinician and the patient, both of which are important for a successful treatment outcome. [45–48]
Conclusion
Chiropractic Maintenance Care reduces the number of days of bothersome (activity-limiting) pain within each new LBP episode among patients classified as dysfunctional (by the MPI-S instrument). MC stabilizes the clinical course and increases the number of pain-free weeks between episodes. Understanding how subgroups of patients are likely to be affected by MC may help align patients’ and clinicians’ expectations with realistic outcomes and can be used as a framework in the selection and execution of appropriate care plans. MC is not a cure that prevents new episodes but rather a management strategy that reduces bothersome (activity-limiting) pain over time for a carefully selected group of patients with recurrent and persistent LBP.
Supplementary information
Additional file 1 Pain trajectories around visits, difference in mean (adjusted) number of days with bothersome pain between groups (Control – MC, 0–7).Contributions
Andreas Eklund was the corresponding author and involved in conceptualization, data curation, formal analysis, funding acquisition, investigation, methodological development, project administration, validation, visualization, writing the original draft, reviewing and editing the final manuscript. Irene Jensen was involved in conceptualization, methodological development, supervision, reviewing and editing the final manuscript. Charlotte Leboeuf-Yde was involved in conceptualization, methodological development, reviewing and editing the final manuscript. Alice Kongsted was involved in conceptualization, methodological development, reviewing and editing the final manuscript. Mattias Jonsson was involved in conceptualization, project administration, reviewing and editing the final manuscript. Peter Lövgren involved in conceptualization, project administration, reviewing and editing the final manuscript. Jakob Petersen-Klingberg involved in conceptualization, project administration, reviewing and editing the final manuscript. Christian Calvert involved in conceptualization, project administration, reviewing and editing the final manuscript. Iben Axén was involved in conceptualization, funding acquisition, methodological development, project administration, supervision, reviewing and editing the final manuscript. The author(s) read and approved the final manuscript.
Competing interests
Five of the authors are paid employees of commercial companies. Andreas Eklund works 40% as a clinician at Hälsan Östertälje Praktikertjänst AB, Södertälje, Sweden. Mattias Jonsson works as a clinician at Ledakuten AB, Lidköping, Sweden. Peter Lövgren works as a clinician at Lövgrens Chiropraktorklinik, Stockholm, Sweden. Jakob Petersen-Klingberg works as a clinician at Eureka Kiropraktik, Borlänge, Sweden. Christian Calvert works as a clinician at Activate Rörelsekliniken, Falkenberg, Sweden. None of these affiliations influenced the study design, data collection and analysis, decision to publish, or preparation of the manuscript. There are no patents, products in development or marketed products associated with this research to declare.
Abbreviations:
LBP: = Low Back Pain MC: = Chiropractic maintenance care MPI-S: = Swedish version of West Haven-Yale Multidimensional Pain Inventory
References
Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, et al.
A systematic review of the global prevalence of low back pain.
Arthritis Rheum. 2012;64(6):2028–37.Hoy, D, March, L, Brooks, P et al.
The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 study
Annals of Rheumatic Diseases 2014 (Jun); 73 (6): 968–974Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, Ferreira PH, Fritz JM.
Prevention and Treatment of Low Back Pain: Evidence, Challenges, and Promising Directions
Lancet. 2018 (Jun 9); 391 (10137): 2368–2383Steffens D, Maher CG, Pereira LS, et al.
Prevention of Low Back Pain: A Systematic Review and Meta-analysis
JAMA Intern Med. 2016 (Feb); 176 (2): 199–208Rubinstein SM, De Zoete A, Van Middelkoop M, Assendelft WJJ, De Boer MR, Van Tulder MW.
Benefits and Harms of Spinal Manipulative Therapy for the Treatment of Chronic Low Back Pain:
Systematic Review and Meta-analysis of Randomised Controlled Trials
British Medical Journal 2019 (Mar 13); 364: l689Oliveira CB, Maher CG, Pinto RZ, Traeger AC, Lin CC, Chenot JF, et al.
Clinical practice guidelines for the management of non-specific low back pain in primary care:
an updated overview.
European Spine Journal 2018;27(11):2791–803.Hong JY, Song KS, Cho JH, Lee JH.
An updated overview of low Back pain Management in Primary Care.
Asian Spine J. 2017;11(4):653–60.Stochkendahl MJ, Kjaer P, Hartvigsen J et al.
National Clinical Guidelines for Non-surgical Treatment of Patients with
Recent Onset Low Back Pain or Lumbar Radiculopathy
European Spine Journal 2018 (Jan); 27 (1): 60–75National Institute for Health and Care Excellence (NICE):
Low Back Pain and Sciatica in Over 16s: Assessment and Management (PDF)
NICE Guideline, No. 59 2016 (Nov): 1–1067Axen I, Jensen IB, Eklund A, Halasz L, Jorgensen K, Lange F, Lovgren PW, Rosenbaum A, Leboeuf-Yde C:
The Nordic Maintenance Care Program: When Do Chiropractors Recommend
Secondary and Tertiary Preventive Care For Low Back Pain?
Chiropractic & Osteopathy 2009 (Jan 22); 17: 1Breen A.
Chiropractic in Britain.
Ann Swiss Chiropractors' Assoc. 1976;6:207–18.Mitchell M.
Maintenance care. Some conciderations.
ACA J Chiropractic. 1980;17:53–5.Sandnes KF, Bjornstad C, Leboeuf-Yde C, Hestbaek L:
The Nordic Maintenance Care Program - Time Intervals Between Treatments of Patients
With Low Back Pain: How Close and Who Decides?
Chiropractic & Osteopathy 2010 (Mar 8); 18: 5Myburgh C, Brandborg-Olsen D, Albert H, Hestbaek L.
The Nordic Maintenance Care Program: What Is Maintenance Care?
Interview Based Survey of Danish Chiropractors
Chiropractic & Manual Therapies 2013 (Aug 20); 21: 27Top Moller L, Hansen M, Leboeuf-Yde C:
The Nordic Maintenance Care Program – An Interview Study on the Use of Maintenance Care
in a Selected Group of Danish Chiropractors
Chiropractic & Osteopathy 2009 (Jun 17); 17: 5Malmqvist S, Leboeuf-Yde C.
The Nordic Maintenance Care Program: Case Management of Chiropractic Patients with
Low Back Pain – Defining the Patients Suitable for Various Management Strategies
Chiropractic & Osteopathy 2009 (Jul 12); 17: 7Leboeuf-Yde C, Hestbaek L:
Maintenance Care In Chiropractic – What Do We Know?
Chiropractic & Osteopathy 2008 (May 8); 16: 3Hansen SF, Laursen ALS, Jensen TS, Leboeuf-Yde C, Hestbaek L:
The Nordic Maintenance Care Program: What Are The Indications For
Maintenance Care In Patients With Low Back Pain? A Survey
of the Members of the Danish Chiropractors' Association
Chiropractic & Osteopathy 2010 (Sep 1); 18: 25Bringsli M, Berntzen A, Olsen DB, Leboeuf-Yde C, Hestbaek L.
The Nordic Maintenance Care Program: Maintenance Care - What Happens During the Consultation?
Observations and Patient Questionnaires
Chiropractic & Manual Therapies 2012 (Aug 10); 20 (1): 25Axen I, Rosenbaum A, Eklund A, Halasz L, Jorgensen K, Lovgren PW, Lange F, Leboeuf-Yde C.
The Nordic Maintenance Care Program – Case Management of Chiropractic Patients With
Low Back Pain: A Survey of Swedish Chiropractors
Chiropractic & Osteopathy 2008 (Jun 18); 16: 6Axen I, Bodin L.
The Nordic Maintenance Care Program: The Clinical Use of Identified Indications for Preventive Care
Chiropractic & Manual Therapies 2013 (Mar 6); 21: 10Eklund A, Axen I, Kongsted A, Lohela-Karlsson M, Leboeuf-Yde C, Jensen I.
Prevention of Low Back Pain: Effect, Cost-effectiveness, and Cost-utility of Maintenance Care -
Study Protocol for a Randomized Clinical Trial
Trials. 2014 (Apr 2); 15: 102Eklund, A., I. Jensen, M. Lohela-Karlsson, J. Hagberg, C. Leboeuf-Yde, et al. (2018).
The Nordic Maintenance Care Program: Effectiveness of Chiropractic
Maintenance Care Versus Symptom-guided Treatment for Recurrent and
Persistent Low Back Pain - A Pragmatic Randomized Controlled Trial
PLoS One. 2018 (Sep 12); 13 (9): e0203029Eklund A, Jensen I, Leboeuf-Yde C, Kongsted A, Jonsson M, Lovgren P, et al.
The Nordic Maintenance Care Program: Does Psychological Profile Modify the Treatment Effect
of a Preventive Manual Therapy Intervention? A Secondary Analysis of a
Pragmatic Randomized Controlled Trial
PLoS One. 2019 (Oct 10); 14 (10): e0223349Kerns RD, Turk DC, Rudy TE.
The west haven-Yale multidimensional pain inventory (WHYMPI).
Pain. 1985;23(4):345–56.Bergstrom C, Hagberg J, Bodin L, Jensen I, Bergstrom G.
Using a psychosocial subgroup assignment to predict sickness absence in a working population
with neck and back pain.
BMC Musculoskelet Disord. 2011;12:81.Bergstrom G, Bergstrom C, Hagberg J, Bodin L, Jensen I.
A 7-year follow-up of multidisciplinary rehabilitation among chronic neck and back pain patients.
Is sick leave outcome dependent on psychologically derived patient groups?
Eur J Pain. 2010;14(4):426–33.Bergstrom G, Bjorklund C, Fried I, Lisspers J, Nathell L, Hermansson U, et al.
A comprehensive workplace intervention and its outcome with regard to lifestyle, health and sick leave:
the AHA study.
Work. 2008;31(2):167–80.Bergstrom G, Jensen IB, Bodin L, Linton SJ, Nygren AL.
The impact of psychologically different patient groups on outcome after a vocational rehabilitation program
for long-term spinal pain patients.
Pain. 2001;93(3):229–37.de Vet HC, Heymans MW, Dunn KM, Pope DP, van der Beek AJ, Macfarlane GJ, et al.
Episodes of low back pain: a proposal for uniform definitions to be used in research.
Spine (Phila Pa 1976). 2002;27(21):2409–16.Eklund A, Jensen I, Lohela-Karlsson M, Leboeuf-Yde C, Axen I.
Absence of Low Back Pain to Demarcate an Episode: A Prospective Multicentre Study in Primary Care
Chiropractic & Manual Therapies 2016 (Feb 18); 24: 3Leboeuf-Yde C, Lemeunier N, Wedderkopp N, Kjaer P.
Absence of Low Back Pain in Patients Followed Weekly Over One Year with Automated Text Messages
Chiropractic & Manual Therapies 2012 (Mar 29); 20: 9Leboeuf-Yde C, Lemeunier N, Wedderkopp N, Kjaer P.
Absence of low back pain in the general population followed fortnightly over one year
with automated text messages.
Chiropr Man Therap. 2014;22(1):1.Axen I, Jones JJ, Rosenbaum A, Lovgren PW, Halasz L, Larsen K, et al.
The Nordic Back Pain Subpopulation Program: Validation and Improvement of a Predictive Model
for Treatment Outcome in Patients With Low Back Pain Receiving Chiropractic Treatment
J Manipulative Physiol Ther. 2005 (Jul); 28 (6): 381–385Leboeuf-Yde C, Gronstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson O, et al.
The Nordic Back Pain Subpopulation Program: Demographic and Clinical Predictors for Outcome
in Patients Receiving Chiropractic Treatment for Persistent Low–Back Pain
J Manipulative Physiol Ther. 2004 (Oct); 27 (8): 493–502Malmqvist S, LeBoeuf-Yde C, Ahola T, Andersson O, Ekström K, Pekkarinen H, Turpeinen M, Wedderkopp N:
The Nordic Back Pain Subpopulation Program:
Predicting Outcome Among Chiropractic Patients in Finland
Chiropractic & Osteopathy 2008 (Nov 7); 16: 13Axen I, Rosenbaum A, Robech R, Larsen K, Leboeuf-Yde C.
Can Patient Reactions to the First Chiropractic Treatment Predict Early Favorable Treatment Outcome
in Nonpersistent Low Back Pain?
J Manipulative Physiol Ther. 2002 (Sep); 25 (7): 450–454Johansen B, Wedderkopp N.
Comparison between data obtained through real-time data capture by SMS and a retrospective telephone interview.
Chiropractic Osteopathy. 2010;18(1):10.Kristjansdottir O, Fors E, Eide E, Finset A, van Dulmen S, Wigers S, et al.
Written online situational feedback via mobile phone to support self-management of chronic widespread pain:
a usability study of a web-based intervention.
BMC Musculoskelet Disord. 2011;12(1):51.SMS-Track. [Available from: http://.www.sms-track.com.
Sandnes KF, Bjornstad C, Leboeuf-Yde C, Hestbaek L:
The Nordic Maintenance Care Program - Time Intervals Between Treatments of Patients
With Low Back Pain: How Close and Who Decides?
Chiropractic & Osteopathy 2010 (Mar 8); 18: 5Kongsted A, Leboeuf-Yde C.
The Nordic Back Pain Subpopulation Program: Course Patterns Established Through Weekly
Follow-ups in Patients Treated For Low Back Pain
Chiropractic & Osteopathy 2010 (Jan 15); 18: 2Kongsted A, Kent P, Axen I, Downie AS, Dunn KM.
What Have We Learned From Ten Years of Trajectory Research in Low Back Pain?
BMC Musculoskelet Disord. 2016 (May 21); 17 (1): 220Menezes Costa CL, Maher CG, Hancock MJ, McAuley JH, Herbert RD, Costa LO.
The prognosis of acute and persistent low-back pain: a meta-analysis.
CMAJ. 2012;184.Ferreira PH, Ferreira ML, Maher CG, Refshauge KM, Latimer J, Adams RD.
The therapeutic Alliance between clinicians and patients predicts outcome in chronic low Back pain.
Phys Ther. 2013;93(4):470–8.Fuentes J, Armijo-Olivo S, Funabashi M, Miciak M, Dick B, Warren S, et al.
Enhanced therapeutic Alliance modulates pain intensity and muscle pain sensitivity in patients with
chronic low Back pain: an experimental controlled study.
Phys Ther. 2014;94(4):477–89.Hall AM, Ferreira PH, Maher CG, Latimer J, Ferreira ML.
The influence of the therapist-patient relationship on treatment outcome in physical rehabilitation:
a systematic review.
Phys Ther. 2010;90(8):1099–110.Lambers NM, Bolton JE.
Perceptions of the quality of the therapeutic alliance in chiropractic care in the Netherlands:
a cross-sectional survey.
Chiropractic Manual Ther. 2016;24.
Return to MAINTENANCE CARE
Return to OUTCOME ASSESSMENT
Since 4-22-2020
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |