Shoulder Dislocation in Young Athletes
Current Concepts in Management
Maxwell C. Park, MD
Theodore A. Blaine, MD
William N. Levine, MD
THE PHYSICIAN AND SPORTSMEDICINE - VOL 30 - NO. 12 - DECEMBER 2002
In Brief: A fall onto an outstretched arm or a collision on the playing field often leads to an acute anterior shoulder dislocation for high school- and college-age athletes. The diagnosis is usually made by history and physical exam. The angle of impact is an important diagnostic clue. If no neurologic contraindications or signs of acute fracture are seen, radiographs are unnecessary, and early reduction before the onset of muscle spasm is essential. Recent advances in arthroscopic techniques have dramatically reduced the high incidence of recurrent instability in young elite athletes, though nonoperative management with immobilization is still an excellent option.
The shoulder is the most commonly dislocated major joint following severe trauma, such as a collision or a fall onto an outstretched arm. The arm is dislocated most often when in abduction and external rotation, as seen in football, basketball, and wrestling. Anterior dislocations account for nearly 95% of all shoulder dislocations. [1] Males are affected much more often than females, especially active adolescents and adults who are younger than age 25.
The natural history of shoulder dislocations in young athletes has been well studied. Recurrent instability following nonoperative treatment ranges from 50% to 100%. [1-5] Primary care physicians need to know general concepts of shoulder instability, including nonoperative management of acute injuries, and recent advances in arthroscopic techniques that have dramatically changed the natural history of this difficult problem.
Normal Anatomy
Shoulder stability is provided by an interrelated, complex array of static and dynamic joint components. [6] Static restraints include the bony articulation (minimal), the glenoid labrum, the capsule and the glenohumeral ligaments, and a negative intra-articular pressure that creates a relative vacuum. [1, 7] The dynamic stabilizers include the rotator cuff, biceps, and scapular muscles. [1, 8, 9]
The labrum is a fibrocartilaginous structure that deepens the surface area of the glenoid fossa by nearly 50% [10] and also serves as the insertion point for the glenohumeral ligaments. Several recent basic science studies on the labrum [11] and glenohumeral ligaments [12-14] have dramatically improved our understanding of shoulder stability. The glenohumeral ligaments are lax through midrange shoulder motion, while the dynamic stabilizers provide most stability; however, in extremes of motion, the glenohumeral ligaments serve as the primary restraints to dislocation.
The superior glenohumeral ligament provides the primary restraint to inferior translation. The middle glenohumeral ligament resists anterior translation in external rotation and less than 45° of abduction; however, the inferior glenohumeral ligament is the most important static stabilizer of the glenohumeral joint. The anterior band serves as the primary restraint to anterior translation in external rotation and abduction (45° or more), [13] as in the cocking phase of pitching. The posterior band provides the primary restraint in flexion, adduction, and internal rotation, [13] as occurs in the release phase of pitching.
Pathologic Processes
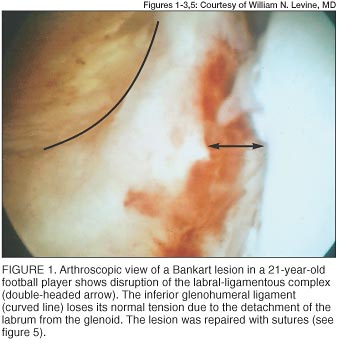 |
Traumatic anterior shoulder dislocations disrupt the labrum and the attached inferior glenohumeral ligament in more than 90% of cases [2, 3, 7, 15-17] (Figure 1). Bankart first brought attention to this finding, calling it the "essential lesion," which now bears his name. [17]
Bigliani et al [18] have shown that plastic deformation of the capsule and ligaments often occurs even in classic Bankart lesions. The capsule failed on the glenoid side (Bankart lesion) in 40%, in midsubstance in 35%, and at the humeral attachment site in 25% of specimens. However, all specimens demonstrated plastic deformation prior to failure. Such deformation can increase capsular laxity, which has been associated with recurrent instability.
The other major pathologic sequela of the dislocated shoulder is a Hill-Sachs lesion. This is an impression defect (fracture) of the posterolateral humeral head as it becomes impacted on the anteroinferior glenoid rim. The shoulder is more unstable with larger defects, because the defect will engage in external rotation, causing the shoulder to dislocate and lock in that position.
Instability can be classified by its direction (anterior, posterior, multidirectional), degree (subluxation, dislocation), cause (traumatic, atraumatic, overuse), or timing (acute, recurrent, fixed). The popular acronyms TUBS (traumatic unidirectional Bankart surgery) and AMBRI (atraumatic multidirectional bilateral rehabilitation inferior capsular shift) have been used, but we avoid them because many patients do not fit neatly into one category or the other. For example, after a fall some athletes who have traumatic dislocations have underlying ligamentous laxity, while some athletes with multidirectional instability may have a traumatic Bankart lesion.
History and Physical Exam Basics
The history and physical exam are crucial elements in the treatment of shoulder instability. The presentation is usually not subtle if an athlete sustains an acute dislocation during a game. However, it is imperative to determine the arm position at the moment of injury, the amount of force used, and the number of previous dislocations. Also, the age at the time of the first dislocation is perhaps the most important prognostic indicator for athletes who have recurrent dislocations. [4]
The physical examination should confirm any suspicions obtained from the history. In the acute setting, a patient usually reports severe pain and holds the arm at the side. The normal contour of the deltoid and acromion are usually lost following anterior dislocations. Assessment includes visual inspection, palpation, strength testing, and a thorough neurovascular examination.
Specific neurologic testing should include premanipulation evaluation of the axillary, musculocutaneous, median, ulnar, and radial nerves. Sensation over the axillary nerve distribution (lateral aspect of the shoulder) is unreliable. In the acute setting, the patient will often have a great deal of pain, making the examination more difficult. However, isometric contraction of the three deltoid heads (anterior, middle, and posterior) usually indicates an intact axillary nerve.
Manual Tests
Information gathered from several manual tests will help determine the extent of the injury.

Apprehension and relocation. Patients who have recurrent instability will often have a positive apprehension test. The classic apprehension maneuver is performed by placing the affected arm in abduction, extension, and external rotation, then applying a gentle anterior translational force (Figure 2A). The apprehension of impending instability is relieved by the relocation test (Figure 2B). If the patient complains of pain alone, then other diagnoses, such as internal impingement, should be considered.
Translation. With the patient supine, anteroposterior (AP) translation is evaluated in 45° of abduction with the shoulder in the plane of the scapula, 30° of flexion, and neutral rotation. An axial force is applied with the examining hand centering the humeral head in the glenoid fossa. The other hand then applies a gentle anterior force to evaluate translation.
Normal translation is 50% of the width of the glenoid surface anteriorly and posteriorly. Translation to the glenoid rim is graded as 1+. Grade 2+ occurs when the head subluxates beyond the rim but self-reduces when the force is released. Grade 3+ entails head dislocation that does not spontaneously reduce. [19]
Inferior stability is assessed with the sulcus test by applying an inferior force to the humerus with the arm at the side. The sulcus exists between the acromion and the inferiorly subluxated humeral head. Translations of 1 cm, 2 cm, or greater than 2 cm are graded as 1+, 2+, and 3+, respectively. [19]
Laxity. Ligamentous laxity is determined by evaluating hyperextension of the elbows, wrists, thumbs, and metacarpophalangeal joints. Assessing ligamentous laxity is critical, because patients who have positive signs may not be appropriate candidates for arthroscopic repair.
Radiographic Findings
 |
In the emergency department, a true AP, transscapular Y, and axillary views should be obtained to determine the direction of the dislocation (Figure 3). A scapular lateral view will confirm an anterior dislocation. Radiographs should be obtained before reduction is attempted unless the direction of dislocation is known from prior dislocations and an experienced physician performs the maneuver. Postreduction radiographs should confirm that the reduction was successful and that there are no acute fractures.
Several special views may be more helpful in athletes who have recurrent instability. The AP radiograph in internal rotation and the Stryker-Notch view are used for documenting Hill-Sachs lesions. The West Point axillary view more clearly outlines the anteroinferior glenoid, thereby avoiding superimposition of the coracoid process and the clavicle. [20]
Secondary studies such as computed tomography and magnetic resonance imaging (MRI) are rarely necessary but can provide valuable information regarding bony pathology (glenoid rim fractures) and capsulolabral injuries.
Open or Closed Reduction?
Based on the history, physical exam, test results, and x-rays, the diagnosis of a dislocated shoulder is fairly straightforward. Most anterior dislocations are treated successfully with closed reduction. Open reduction may be indicated if associated fractures are evident or if inadequate muscle relaxation prohibits a closed reduction.
After a thorough neurologic examination with special attention to the axillary and musculocutaneous nerves, acute anterior shoulder dislocation may be reduced on the playing field prior to obtaining radiographs. The practitioner applies gentle longitudinal traction to the humerus while gradually flexing the arm forward to allow for relocation of the humeral head. It may be possible to perform the reduction acutely before the onset of muscle spasm and pain. If a fracture is suspected (eg, crepitus on palpation, immediate swelling, or ecchymosis), then reduction attempts should not be performed before obtaining radiographs.
Many techniques have been described for in-office reduction, and all of them rely on muscle relaxation and pain management, which traditionally has required intravenous sedation, analgesics, and cardiovascular monitoring. However, one report [21] documented the efficacy of 20 mL of 1% lidocaine hydrochloride injected into the shoulder joint and allowed to settle for 5 to 10 minutes. When the patient is comfortable, a closed reduction can be performed.
Stimson's method uses traction to allow a gentle reduction. With the patient prone, the affected arm is extended vertically from the exam table, and a 10- to 15-lb weight is applied to the forearm and wrist. It may take up to 20 minutes to achieve reduction with this technique.
The traction-countertraction technique is also safe and effective. An assistant applies countertraction by pulling a sheet or strap that has been wrapped around the patient's torso to stabilize the chest and scapula. The physician pulls and gently rotates the extremity to unhinge the dislocated humeral head (Figure 4).
The forward elevation maneuver is performed with the patient supine on the examination table. Acetaminophen with codeine may be given orally 20 minutes before the maneuver. Intravenous drugs are usually not required unless the patient is uncooperative or numerous previous attempts have been unsuccessful. The arm is slowly elevated 10° to 20° in forward flexion and slight abduction; forward flexion is continued until the arm is directly overhead. In this position, or at 90° of forward flexion, the examiner increases abduction while applying careful upward and outward traction. The humeral head is displaced beneath the coracoid and brought to the edge of the glenoid. If the shoulder is not reduced by this point, internal rotation with gentle pressure to the humeral head by the physician's thumb will complete the reduction. [22]
The scapular manipulation technique requires the patient to be prone with the shoulder in 90° of forward flexion and external rotation. The forearm is suspended from the table with the wrist secured and the elbow flexed. Traction is maintained with 5 to 15 lb for 5 minutes. With the patient relaxed, the physician pushes medially on the tip of the scapula (lifting it occasionally), while laterally rotating the superior aspect of the scapula. A palpable clunk signals reduction. [23]
It is imperative to document the neurologic examination before and after reduction to rule out brachial plexus or peripheral nerve injuries. Postreduction radiographs should also be obtained.

Nonoperative Treatment Regimen
After reduction, a sling is used to immobilize the shoulder in adduction and internal rotation. Recently, immobilization of the affected arm in external rotation has been advocated. This position has been shown by MRI to better maneuver the Bankart lesion toward the glenoid neck than conventional internal rotation. [24] Further study is required to elucidate the clinical ramifications of immobilization in external rotation.
The duration of immobilization has been controversial, but 3 to 6 weeks is recommended. [1, 17] Ideally, immobilization will allow a fibroblastic response to damaged tissue. Rotational and scapular strengthening exercises are then instituted under close physician and physical therapist supervision. The program normalizes strength and motion with progressive resistance training. The provocative position of abduction and external rotation is avoided for at least 6 weeks. Return to sports is allowed when the young athlete has a full and pain-free range of motion, normal strength, and little or no apprehension. [1]
Despite immobilization, supervised rehabilitation, and gradual return to full activity, dislocation recurrence ranges from 60% to 94% in patients younger than 25. [1-5] Marans et al [25] documented recurrence rates as high as 100%, regardless of the immobilization period. As a result, immediate surgery without an initial trial of rehabilitation has been advocated for young, elite athletes. [2, 3, 15]
Recent Treatment Advances
If surgery is required, an open procedure or arthroscopic technique must be chosen. For patients who have recurrent dislocations, arthroscopic techniques have resulted in higher recurrence rates than open procedures. [15, 16, 26] Possible explanations for the higher recurrence rate include capsular redundancy, inadequate fixation techniques, bony deficiency, and subsequent contact sports. Thus, recent interest in arthroscopic procedures for anterior stabilization of the shoulder has shifted from recurrent shoulder dislocations to treatment for acute dislocations, especially in young athletes. [1-3, 25]
 |
Arthroscopic Bankart repair. In a prospective, nonrandomized study of patients with first-time dislocations, [2] 21 West Point cadets were treated with arthroscopic Bankart repair within 10 days of injury, and 15 cadets were treated with immobilization for 4 weeks. Twelve of the 15 (80%) nonoperatively treated cadets had recurrent instability, but only 3 of 21 (14%) operatively treated cadets did. Two of these events occurred in patients who experienced one-time subluxations requiring no further treatment; the other patient experienced a recurrent dislocation and subsequently underwent open stabilization.
Tacks and sutures. In a more recent study of first-time dislocations, [3] 19 cadets were treated with arthroscopically placed bioabsorbable tacks. At a minimum follow-up of 2 years, only one (5%) recurrent dislocation occurred. However, questions have been raised about the tacks used in this initial study. Sterile synovitis, painful clicking of the humeral head over the tack, tack head avulsion, and the nonanatomic repair of the tissue because of the medial placement of the tack on the scapular neck have been reported. With the development of improved techniques and technology, the arthroscopic procedure can now be done the same way as the open procedure. Suture fixation of the torn labral-ligamentous complex more reliably reattaches the structures to their anatomic position (Figure 5). In addition, proper retensioning of the complex is more reproducible with sutures than with first-generation tacks.
Thermal capsular shrinkage. The development of a radiofrequency heat probe for capsular shrinkage has created interest in its potential use as an adjunct for arthroscopic stabilization of shoulder dislocations. Treating unaddressed capsular laxity with heat-generated shrinkage of the collagen in the capsule and glenohumeral ligaments is particularly appealing as an adjunct to Bankart repair. Although this technique has been available as an arthroscopic treatment option for 5 years, great caution should be exercised in its use. Reports of axillary motor and sensory neuropathy, obliteration of the joint capsule, and failure of the thermal capsular shrinkage procedure at an alarmingly high rate have raised concern about potential widespread use. Inconsistent tissue response related to patient age has also been a problem in some instances. Specific indications have not been elucidated fully because long-term outcomes are yet to be published in the medical literature. [27]
Open Bankart reconstruction. Most young athletes who have recurrent anterior shoulder instability and require surgery will need open Bankart reconstruction with capsular shift. In this surgical procedure, the subscapularis muscle is removed from its insertion on the lesser tuberosity, and the underlying capsule is then reflected from its humeral insertion. The medial capsulolabral injury (Bankart lesion) can then be reattached directly back to the bone. In addition, capsular shift (imbrication of the capsule) can be titrated based on the amount of intraoperative capsular redundancy found by the surgeon. This is an excellent procedure for most young athletes who have recurrent shoulder instability. However, this procedure may not be suitable for elite overhead athletes, because loss of the terminal 3° to 5° of external rotation may be catastrophic in terms of the patient's athletic performance.
Current Treatment Recommendations
Careful history, physical examination, and radiographic evaluation are essential in accurately diagnosing dislocated shoulders. Traditional methods of nonoperative treatment, including reduction of the dislocation, immobilization, and strengthening exercises, have been inconsistent in eliminating recurrent dislocations, which are problematic for any athlete, not just those who compete at elite levels. This has led to recent studies demonstrating the efficacy of early operative intervention in the treatment of first-time dislocations in young, active patients and excellent results of open repair for recurrent instability.
Although arthroscopic treatment of recurrent instability has yielded less favorable outcomes, it has produced outstanding results for first-time dislocations. As the technology has evolved, the procedure more closely resembles the open technique, and, not surprisingly, results have improved. Initial excitement in the radiofrequency probe led to its widespread use over the last several years. However, the results thus far have been disappointing, and long-term follow-up is required before this procedure can be recommended for widespread use.
References:
Hawkins RJ, Mohtadi NG:
Controversy in anterior shoulder instability.
Clin Orthop 1991;272(Nov):152-161
Arciero RA, Wheeler JH, Ryan JB, et al:
Arthroscopic Bankart repair versus nonoperative treatment for acute, initial anterior shoulder dislocations.
Am J Sports Med 1994;22(5):589-594
Arciero RA, Taylor DC, Snyder RJ, et al:
Arthroscopic bioabsorbable tack stabilization of initial anterior shoulder dislocations: a preliminary report.
Arthroscopy 1995;11(4):410-417
Hovelius L, Augustini BG, Fredin H, et al:
Primary anterior dislocation of the shoulder in young patients: a ten-year prospective study.
J Bone Joint Surg Am 1996;78(11):1677-1684
Henry JH, Genung JA:
Natural history of glenohumeral dislocation--revisited.
Am J Sports Med 1982;10(3):135-137
Kvitne RS, Jobe FW:
The diagnosis and treatment of anterior instability in the throwing athlete.
Clin Orthop 1993;291(Jun):107-123
Moseley HF, Övergaard B:
The anterior capsular mechanism in recurrent anterior dislocation of the shoulder: morphological and clinical studies with special reference to the glenoid labrum and the gleno-humeral ligaments.
J Bone Joint Surg Br 1962;44(4):913
Howell SM, Imobersteg AM, Seger DH, et al:
Clarification of the role of the supraspinatus muscle in shoulder function.
J Bone Joint Surg Am 1986;68(3):398-404
Perry J:
Anatomy and biomechanics of the shoulder in throwing, swimming, gymnastics and tennis.
Clin Sports Med 1983;2(2):247-270
Howell SM, Galinat BJ:
The glenoid-labral socket: a constrained articular surface.
Clin Orthop 1989;243(Jun):122-125
Flatow EL, Warner JJP:
Instability of the shoulder: complex problems and failed repairs. Part 1: relevant biomechanics, multidirectional instability, and severe loss of glenoid and humeral bone
J Bone Joint Surg Am 1998;80(1):122-140
Ticker JB, Bigliani LU, Soslowsky LJ, et al:
Inferior glenohumeral ligament: geometric and strain-rate dependent properties.
J Shoulder Elbow Surg 1996;5(4):269-279
Turkel SJ, Panio MW, Marshall JL:
Stabilizing mechanisms preventing anterior dislocation of the glenohumeral joint.
J Bone Joint Surg Am 1981;63(8):1208-1217
O'Connell PW, Nuber GW, Mileski RA, et al:
The contribution of the glenohumeral ligaments to anterior stability of the shoulder joint.
Am J Sports Med 1990;18(6):579-584
Liu SH, Henry MH:
Anterior shoulder instability: current review.
Clin Orthop 1996;323(Feb):327-337
Grana WA, Buckley PD, Yates CK:
Arthroscopic Bankart suture repair.
Am J Sports Med 1993;21(3):348-353
Rowe CR, Patel D, Southmayd WW:
The Bankart procedure: a long-term end-result study.
J Bone Joint Surg Am 1978;60(1):1-16
Bigliani LU, Pollock RG, Soslowsky LJ, et al:
Tensile properties of the inferior glenohumeral ligament.
J Orthop Res 1992;10(2)187-197
Altchek DW, Warren RF, Skyhar MJ, et al:
T-plasty modification of the Bankart procedure for multidirectional instability of the anterior and inferior types.
J Bone Joint Surg Am 1991;73(1):105-112
Rokous JR, Feagin JA, Abbott HG:
Modified axillary roentgenogram: a useful adjunct in the diagnosis of recurrent instability of the shoulder.
Clin Orthop 1972;82(Jan-Feb):84-86
Matthews DE, Roberts T:
Intraarticular lidocaine versus intravenous analgesic for reduction of acute anterior shoulder dislocations: a prospective randomized study.
Am J Sports Med 1995;23(1):54-58
Janecki CJ, Shahcheragh GH:
The forward elevation maneuver for reduction of anterior dislocations of the shoulder.
Clin Orthop 1982;164(Apr):177-180
Anderson D, Zvirbulis R, Ciullo J:
Scapular manipulation for reduction of anterior shoulder dislocations.
Clin Orthop 1982;164(Apr):181-183
Itoi E, Sashi R, Minagawa H, et al:
Position of immobilization after dislocation of the glenohumeral joint: a study with use of magnetic resonance imaging.
J Bone Joint Surg Am 2001;83(5):661-667
Marans HJ, Angel KR, Schemitsch BH, et al:
The fate of traumatic anterior dislocation of the shoulder in children.
J Bone Joint Surg Am 1992;74(8):1242-1244
Steinbeck J, Jerosch J:
Arthroscopic transglenoid stabilization versus open anchor suturing in traumatic anterior instability of the shoulder.
Am J Sports Med 1998;26(3):373-378
Abrams JS:
Thermal capsulorrhaphy for instability of the shoulder: concerns and applications of the heat probe.
Instr Course Lect 2001;50:29-36
Dr Park is a resident, Dr Blaine is an assistant professor, and Dr Levine is an assistant professor of orthopedic surgery and director of sports medicine at Columbia-Presbyterian Medical Center at Columbia University in New York City.
Address correspondence to William N. Levine, MD, Columbia-Presbyterian Medical Center, Center for Shoulder, Elbow and Sports Medicine, 622 W 168th St, PH-1117, New York, NY 10032; e-mail to wnl1@columbia.edu.
Disclosure information: Drs Park, Blaine, and Levine disclose no significant relationship with any manufacturer of any commercial product mentioned in this article. No drug is mentioned in this article for an unlabeled use.
Copyright (C) 2002. The McGraw-Hill Companies. All Rights Reserved
