| |

| 
| |
The Shoulder Page
This section was compiled by Frank M. Painter, D.C.
Send all comments or additions to:
Frankp@chiro.org
If there are terms in these articles you don't understand, you can get a definition from the Merriam Webster Medical Dictionary. If you want information about a specific disease, you can access the Merck Manual. You can also search Pub Med for more abstracts on this, or any other health topic.
|
Jump to:
Primary Shoulder Resources
Shoulder Literature
The Patient's Guide to the Shoulder
|
 |
 |
| |
| |
|
| |
|
|
|
|
| |
| |
|
| |
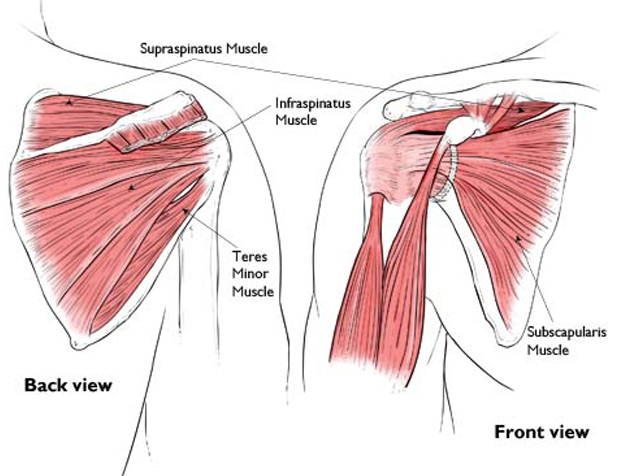
The Shoulder Girdle
Thanks to
ShoulderDoc.UK for access to this picture!
The following illustration clearly shows the four muscles
and the tendons that form the rotator cuff and stabilize the shoulder joint.
Reproduced with permission from The Body Almanac.
(c) American Academy of Orthopaedic Surgeons, 2003.
|
 |
|
|
|
| |
| |
|
| |
|
|
|
| |
| |
|
| |

|
Relationships Between Active Myofascial Trigger Points and Depressive
Symptoms and Physical and Clinical Characteristics of Individuals
With Shoulder Pain: A Cross-sectional Study
European J Pain 2021 (Sep); 25 (8): 1644–1667 ~ FULL TEXT
This study found that MTPs in individuals with shoulder pain contributed to depressive symptoms and pain during internal and external rotation ROM and internal rotation strength test.
|
|
|
Noninvasive Management of Soft Tissue Disorders of the Shoulder:
A Clinical Practice Guideline From the Ontario Protocol
for Traffic Injury Management (OPTIMa) Collaboration
European J Pain 2021 (Sep); 25 (8): 1644–1667 ~ FULL TEXT
Our shoulder guideline provides evidence-based recommendations (i.e., recommendations 3, 4, and 5) to help clinicians deliver effective interventions for the management of soft tissue disorders of the shoulder (excluding major pathology). The recommended interventions aim to promote uniform high-quality care based on systematic reviews of the literature and synthesis of best available evidence. Implementing the evidence-based recommendations for shoulder pain will likely improve patient outcomes, reduce regional variations, and improve the efficiency of the healthcare system (Anis et al., 1995; Nichol et al., 1999; Rutten et al., 2010). Our recommendations on assessment, patient education, and reevaluation and discharge (i.e., recommendations 1, 2, and 6) are based on universal principles of health professions' standards of practice (Hopman et al., 2013; Stiggelbout et al., 2012; Washington State Department of Labor and Industries, 2014).
|
|
|
Shoulder Pain Prevalence by Age and Within
Occupational Groups: A Systematic Review
Archives of Physiotherapy 2021 (Nov 4); 11 (1): 24 ~ FULL TEXT
Shoulder pain was previously shown to diminish in older populations and it was suggested that this could be explained by reduced usage with age. This study found that: Shoulder pain prevalence remains common in workers beyond the age of 50. Prevalence continues to increase in physically demanding occupations. Clinicians should consider factors of occupation when managing shoulder pain.
|
|
|
Validity of Cyriax's Functional Examination for Diagnosing
Shoulder Pain: A Diagnostic Accuracy Study
J Manipulative Physiol Ther. 2019 (Jul); 42 (6): 407–415 ~ FULL TEXT
There was no significant difference between the 2 groups regarding age, sex, and body mass index. Moderate to high sensitivity (74.1%, 76.5%, and 66.7%) and high specificity (93.0%, 99.5%, and 99.0%) were in supraspinatus, subscapularis, and infraspinatus lesions, respectively. For the subacromial-subdeltoid bursitis, high sensitivity (90.4%) and moderate to high specificity (70.3%) was found. In contrast, low sensitivity (15.0%) and high specificity (100.0%) were found in the biceps lesions.
|
|
|
Utilization of Manipulative Treatment for Spine and Shoulder Conditions
Between Different Medical Providers in a Large Military Hospital
Arch Phys Med Rehabil. 2017 (Jul 14) [Epub] ~ FULL TEXT
Of 7,566 total patients seeking care, 2014 (26.6%) received manipulative treatment at least once, and 1,870 of those received this treatment in a military facility (24.7%). Manipulative treatment was used most often for thoracic conditions and least often for shoulder conditions (50.8% and 24.2% of all patients). There was a total of 6,706 unique medical visits with a manipulative treatment procedure (average of 3.3 manipulative treatment procedure visits per patient).
Manipulative treatment utilization rates for shoulder and spine conditions ranged from 26.6% to 50.2%. Chiropractors used manipulation the most and physical therapists the least.
|
|
|
Systematic Review of Nondrug, Nonsurgical Treatment
of Shoulder Conditions
J Manipulative Physiol Ther 2017 (Jun); 40 (5): 293–319 ~ FULL TEXT
Twenty-five systematic reviews and 44 RCTs met inclusion criteria. Low- to moderate-quality evidence supported the use of manual therapies for all 4 shoulder conditions. Exercise, particularly combined with physical therapy protocols, was beneficial for shoulder impingement syndrome (SIS) and adhesive capsulitis (AC). For SIS, moderate evidence supported several passive modalities. For RC, physical therapy protocols were found beneficial but not superior to surgery in the long term. Moderate evidence supported extracorporeal shockwave therapy for calcific tendinitis RC. Low-level laser was the only modality for which there was moderate evidence supporting its use for all 4 conditions.
|

|
First-Contact Care With a Medical vs Chiropractic Provider
After Consultation with a Swiss Telemedicine Provider:
Comparison of Outcomes, Patient Satisfaction, and
Health Care Costs in Spinal, Hip,
and Shoulder Pain Patients
J Manipulative Physiol Ther. 2015 (Sep); 38 (7): 477–483 ~ FULL TEXT
JMPT's Editor-in-Chief Claire Johnson, DC, MEd, emphasized the importance of the latest findings:
“Comparative studies – in other words, research that compares the outcomes between two different providers or modalities – are rare for chiropractic care,” she said. “Thus, this study by Houweling, et al., is especially important if payers and policy-makers are to better understand the 'triple aim' as it relates to chiropractic. Specifically, this study helps us better understand what type of care provides better patient satisfaction, is more cost effective, and improves population health.”
|
|
|
Shoulder Injuries: A Functional Perspective
ACA News 2013 (Aug): 34–35 ~ FULL TEXT
The rotator cuff, as all doctors of chiropractic know, is actually composed of four separate muscles: the supraspinatus, the infraspinatus, the teres minor and the subscapularis. Most of the approximately 2 million people who seek care for rotator cuff injuries in the United States every year have injured the supraspinatus, but the involvement of at least one of the other muscles is more common than was previously thought, says Dale Huntington, DC, owner of the Huntington Chiropractic Clinic in Springdale, Ark. “We used to think these tears were just in the super-spinatus 90 percent of the time. Now we’re realizing that, in the converging of these tendons, the infraspinatus is often being torn as well.”
|
|
|
Manipulative Therapy for Shoulder Pain and Disorders:
Expansion of a Systematic Review
J Manipulative Physiol Ther 2011 (Jun); 34 (5): 314–346 ~ FULL TEXT
This study found a level of B or fair evidence for manual and manipulative therapy (MMT) of the shoulder, shoulder girdle, and/or full kinetic chain (FKC) combined with multimodal or exercise therapy for rotator cuff injuries disease or disorders (RCIDs). There is a fair or B level of evidence for MMT of the shoulder/shoulder girdle and FKC combined with a multimodal treatment approach for shoulder complaints, dysfunction, disorders and/or pain (SCDP). There is a fair (B) level of evidence for MMT with exercise that included proprioceptive retraining as helpful for frozen shoulder (FS) or adhesive capsulitis. There was a fair level of evidence (B) for MMT using soft tissue or myofascial treatments for soft tissue disorders (ST) of the shoulder. There is a limited level of evidence (C) for cervical lateral glide mobilization (CLGM) and/or HVLA manipulation with soft tissue release and exercise in the treatment of minor neurogenic shoulder pain (NSP). There is an insufficient level of evidence (I) for MMT with or without exercise or multimodal therapy in the treatment of OA of the shoulder. In particular, MMT must be combined, when safe, appropriate, and including no contraindications, with commonly indicated exercise or rehabilitative therapy, as it remains the standard care. For clinicians, however, this study is intended to guide them in the appropriate use of MMT, soft tissue technique, exercise, and/or multimodal therapy for the treatment of a variety of shoulder complaints in the context of the entire hierarchy of available evidence.
|
|
|
Manipulative Therapy in Addition to Usual Care
for Patients With Shoulder Complaints:
Results of Physical Examination Outcomes in
a Randomized Controlled Trial
J Manipulative Physiol Ther 2010 (Feb); 33 (2): 96–101 ~ FULL TEXT
The factor analysis resulted in 4 factors: “shoulder pain,” “neck pain,” “shoulder mobility,” and “neck mobility.” At 6 weeks, no significant differences between groups were found. At 12 weeks, the mean changes of all 4 factors favored the intervention group; the factors “shoulder pain” and “neck pain” reached statistical significance (95% confidence interval [CI], 0.1-2.1). At 26 weeks, differences in the factors “shoulder pain” (95% CI, 0.0-2.6), “shoulder mobility” (95% CI, 0.2-1.7), and “mobility neck” (95% CI, 0.2-1.3) statistically favored the intervention group. Manipulative therapy, in addition to usual care by the general practitioner, diminishes the severity of the pain in the shoulder and neck and improves the mobility of the shoulder and the cervicothoracic spine.
|
|
|
A Multi-modal Treatment Approach for the Shoulder:
A Four Patient Case Series
Chiropractic & Osteopathy 2005 (Sep 16); 13 (1): 20 ~ FULL TEXT
The patient underwent a multimodal treatment protocol including soft tissue therapy, phonophoresis, diversified manipulation; and rotator cuff and shoulder girdle muscle exercises. Outcomes included pain measurement; range of motion of the shoulder, and return to normal daily, work, and sporting activities. At the end of the treatment protocol the patient was symptom free with all outcome measures normal. The patient was followed up at 4 and 12 weeks and continued to be symptom free with full range of motion and complete return to normal daily and pre-treatment activities.
|
|
|
Identifying and Managing Shoulder Pain
in Competitive Swimmers
(PDF)
Physician And Sportsmedicine 2005 (Sep); 33 (9) ~ FULL TEXT
Shoulder pain resulting from glenohumeral instability is common among competitive swimmers. The biomechanics inherent to swimming promote muscular imbalances that stress the capsuloligamentous structures and contribute to shoulder instability. Most swimmers respond favorably to conservative treatment of rest and rehabilitation, while a small percentage may ultimately require surgical intervention. Swimmers who respond well to rehabilitation have a better prognosis for a successful return to swimming than those who require surgery. Overall, education in proper stroke and training techniques can minimize the likelihood that a competitive swimmer will experience disabling shoulder pain.
|
|
|
Upper Extremity Rehab in the Elderly
Kim Christensen,DC,DACRB,CCSP,CSCS
Dynamic Chiropractic (April 23, 2005)
There is now a wealth of data that supports the value of resistance exercise in the geriatric population. Improvements are seen in weight and body composition, decreased falls/improved balance, better psychological health, less frailty, and improved function. With exercise, the resting blood pressure lowers and there is a reduction in the risk of all-cause mortality. [3] These benefits overwhelm the few detrimental concerns, and encourage us to recommend resistance exercise to older patients who need upper extremity rehab.
|
|
|
Shoulder Pain and Weakness (PDF)
Physician And Sportsmedicine 2004 (Nov); 32 (11) ~ FULL TEXT
An otherwise healthy 47-year-old man reported a history of right shoulder pain subsequent to an injury he sustained several months earlier while boating. The patient recalled trying to lift a heavy object out of the water when his right arm was forcibly externally rotated. The patient related that his arm was sore for several days after the injury, but his pain receded and became manageable. He did not seek medical care acutely. Months later, when he did seek care, he said that he had lost overall power in his shoulder and had generalized shoulder pain with activity. Furthermore, he could not tuck his shirt into his pants with his right arm.
|
|
|
Rotator Cuff Impingement
J Manipulative Physiol Ther 2004 (Nov); 27 (9): 580–590 ~ FULL TEXT
Outcomes included pain measurement; range of motion of the shoulder, and return to normal daily, work, and sporting activities. At the end of the treatment protocol the patient was symptom free with all outcome measures normal. The patient was followed up at 4 and 12 weeks and continued to be symptom free with full range of motion and complete return to normal daily and pre-treatment activities.
|
|
|
Manipulative Therapy in Addition to Usual Medical Care
for Patients with Shoulder Dysfunction and Pain:
A Randomized, Controlled Trial
Ann Intern Med 2004 (Sep 21); 141 (6): 432–439 ~ FULL TEXT
Manipulative therapy for the shoulder girdle in addition to usual medical care accelerates recovery of shoulder symptoms.
|
|
|
Predictive Factors for Neck and Shoulder Pain:
A Longitudinal Study in Young Adults
SPINE (Phila Pa 1976) 2004 (Aug 1); 29 (15): 1662–1669
This random sample of 826 high school students was investigated when they were 15 to 18 years old, and again at 22 to 25 years of age, to estimate the prevalence and incidence of neck and shoulder pain in young adults, and to identify the associated and predictive factors of neck and shoulder pain based on a 7-year follow-up. In 7 years, the prevalence of weekly neck and shoulder pain increased from 17% to 28%. Among those who were asymptomatic at baseline, 6-month incidence of occasional or weekly neck and shoulder pain was 59% 7 years later. In young adults, the incidence of neck and shoulder pain is high, and the associated factors of neck and shoulder pain are already multifactorial in a young population.
|
|
|
Biomechanical Factors That Contribute To Rotator Cuff Function
And Injury: A Focus on Chiropractic Sports Care
Today's Chiropractic 2004 (May) ~ FULL TEXT
This article reviews the biomechanical structure and function of the glenohumeral joint, the typical mechanisms of injury, and then reviews injury prevention, exercises, and rehabilitative strategies.
|
|
|
NSAIDs and Musculoskeletal Treatment:
What Is the Clinical Evidence?
Physician And Sportsmedicine 2003 (Jan); 31 (1) ~ FULL TEXT
Nonsteroidal anti-inflammatory drugs (NSAIDs) are commonly prescribed for musculoskeletal injuries because the conditions are believed to be inflammatory in nature. However, because inflammation is a necessary component in the healing process, decreasing inflammation may prove counterproductive. Also, many tendon injuries called 'tendinitis' are, in fact, degenerative and not inflammatory conditions. An analysis of the pathophysiology and healing of musculoskeletal injuries questions the use of NSAIDs in many treatment protocols. Because NSAIDs have profound side effects, they should not automatically be the first choice for treating musculoskeletal injuries.
|
|
|
Shoulder Dislocation in Young Athletes
Physician And Sportsmedicine 2002 (Dec); 30 (12) ~ FULL TEXT
A fall onto an outstretched arm or a collision on the playing field often leads to an acute anterior shoulder dislocation for high school- and college-age athletes. The diagnosis is usually made by history and physical exam. The angle of impact is an important diagnostic clue. If no neurologic contraindications or signs of acute fracture are seen, radiographs are unnecessary, and early reduction before the onset of muscle spasm is essential. Recent advances in arthroscopic techniques have dramatically reduced the high incidence of recurrent instability in young elite athletes, though nonoperative management with immobilization is still an excellent option.
|
|
|
Managing Shoulder Sprain/Strain Injuries
Kim Christensen,DC,DACRB,CCSP,CSCS
Dynamic Chiropractic (October 21, 2002)
Many of the shoulder problems that chiropractors see involve one or more forms of rotator mechanism dysfunction. This chronic biomechanical continuum usually begins with dysfunction of the rotator cuff muscles and progresses to rotator cuff syndrome; supraspinatus tendinitis; impingement syndrome; subdeltoid and subacromial bursitis; calcific shoulder bursitis; and even most cases of frozen shoulder and bicipital tendinitis. In such cases, there is no direct, acute injury.
|
|
|
Osteoarthritis of the Glenohumeral Joint:
Nonsurgical Treatment Options
Physician And Sportsmedicine 2002 (Apr); 30 (4) ~ FULL TEXT
Athletes at risk include weight lifters, baseball players, softball players, and those who play racket sports such as tennis, racquetball, and squash. Glenohumeral osteoarthritis (GHOA) seems to result from pure instability, rotator cuff arthropathy, fracture, or postsurgical trauma and predominately affects older men. GHOA generally involves the glenoid rather than the humeral side of the joint,3 which will influence rehabilitation.
|
|
|
Osteoarthritis of the Glenohumeral Joint:
Nonsurgical Treatment Options
Physician And Sportsmedicine 2002 (Apr); 30 (4) ~ FULL TEXT
Athletes at risk include weight lifters, baseball players, softball players, and those who play racket sports such as tennis, racquetball, and squash. Glenohumeral osteoarthritis (GHOA) seems to result from pure instability, rotator cuff arthropathy, fracture, or postsurgical trauma and predominately affects older men. GHOA generally involves the glenoid rather than the humeral side of the joint,3 which will influence rehabilitation.
|
|
|
Chiropractic Management of Shoulder Pain and
Dysfunction of Myofascial Origin Using
Ischemic Compression Techniques
J Can Chiropr Assoc 2002; 46 (3): 192–200 ~ FULL TEXT
Shoulder pain and dysfunction is a chief complaint commonly presenting to a chiropractor’s office. The purpose of this article is to review the most common etiologies of shoulder pain, focusing on those conditions of a myofascial origin. In addition to a review of the literature, the author draws upon his own clinical experience to describe a method to diagnose and manage, patients with shoulder pain of myofascial origin using ischemic compression techniques. This hands-on therapeutic approach conveys several benefits including: positive therapeutic outcomes; a favorable safety profile and; it is minimally strenuous on the doctor and well tolerated by the patient.
|
|
|
Chiropractic Management of a Professional Hockey Player
with Recurrent Shoulder Instability
J Manipulative Physiol Ther 2001 (Jul); 24 (6): 425–430 ~ FULL TEXT
The patient had undergone strength training for rehabilitation after each of the previous two shoulder operations and had very strong rotator cuff and scapular musculature. Proprioceptive testing revealed a poor response in the left shoulder compared with the right shoulder. Two subjective outcome measures were used to determine the effectiveness of the treatment protocol in reducing the symptoms of recurrent shoulder instability. Much of the treatment focused on proprioceptive training, soft tissue mobilization, and improving joint function.
|
|
|
Shoulder Muscle Dysfunction and the Golf Swing:
Important Treatment and Educational Considerations
David Seaman, DC, MS, DABCN and George DeFranca, DC
Dynamic Chiropractic (May 1, 2000)
While watching the golf swing, it's obvious that shoulder muscles are used to create a powerful swing. Not so obvious are the details of shoulder muscle activity during the swing. Fortunately, a handful of electromyographic studies have given us a better understanding of shoulder muscle function during the golf swing. [3, 4, 5] These studies demonstrate that rotator cuff muscles (particularly the subscapularis), the latissimus dorsi and pectoralis major are highly active during the golf swing.
|
|
|
Immobilization or Early Mobilization After
an Acute Soft–Tissue Injury?
Physician And Sportsmedicine 2000 (Mar); 28 (3) ~ FULL TEXT
Acute soft-tissue injuries such as muscle-tendon strains, ligament sprains, and ligament or tendon ruptures occur frequently in sports and exercise. Without correct diagnosis and proper treatment, they may result in long-term breaks in training and competition. Far too often, injuries become chronic and end careers of competitive athletes or force recreational athletes to abandon their favorite activity. For these reasons, an increased focus has been on finding ways to ensure optimal healing. In this regard, the question has centered on immobilization or early mobilization in treatment.
|
|
|
Sports Update: Evaluation of the Unstable Shoulder
Thomas Souza,DC, DACBSP
Dynamic Chiropractic (September 20, 1999)
There has been an explosion of new tests for labrum tears of the shoulder. Among those developed and studied over the last few years have included the Crank test, O'Brien's sign (active compression test) and the anterior slide test. The new biceps load test was designed and tested on patients with recurrent anterior dislocations. This subpopulation may respond differently than patients without a history of dislocation; therefore, extrapolation beyond this population is not recommended.
|
|
|
Comparison of Physiotherapy, Manipulation, and Corticosteroid
Injection for Treating Shoulder Complaints in General Practice:
Randomised, Single Blind Study
British Medical Journal 1997 (May 3); 314 (7090): 1320–1325 ~ FULL TEXT
In the shoulder girdle group duration of complaints was significantly shorter after manipulation compared with physiotherapy (P < 0.001). Also the number of patients reporting treatment failure was less with manipulation. In the synovial group duration of complaints was shortest after corticosteroid injection compared with manipulation and physiotherapy (P < 0.001). Drop out due to treatment failure was low in the injection group (17%) and high in the manipulation group (59%) and physiotherapy group (51%). For treating shoulder girdle disorders, manipulation seems to be the preferred treatment. For the synovial disorders, corticosteroid injection seems the best treatment.
|
|
|
Faulty Movement Patterns as a Cause of Articular Dysfunction
Craig Liebenson, DC
Dynamic Chiropractic – February 10, 1997
During activities involving lifting of the arms, fixation of the scapulae is the key. Upper trapezius and levator scapulae fix the scapulae from above, while the lower trapezius and serratus anterior do so from below. The upper fixators attach to the cervical spine while the lower ones attach to the thoracic spine. Since the upper fixators are usually overactive and the lower fixators inhibited, overstrain of the cervical spine during carrying or reaching activities is common.
|
|
|
Chiropractic Treatment of Frozen Shoulder Syndrome
(Adhesive Capsulitis) Utilizing Mechanical Force,
Manually Assisted Short Lever Adjusting Procedures
J Manipulative Physiol Ther 1995 (Feb); 18 (2): 105–115
The patient's shoulder was conservatively managed with chiropractic adjustments to the affected shoulder joint, as well as to the cervicothoracic spine. Treatment consisted of mechanical force, manually assisted short lever chiropractic adjustments, delivered via an Activator Adjusting Instrument. Successful resolution of the presenting symptomatology was achieved.
|
|
|
|
| |
| |
|
| |
|
The “Patient's Guide” to the Shoulder
|
|
|
|
| |
| |
|
| |
|
Please NOTE that the following series of articles are provided by orthopedic surgeons. They are only listed here because of the anatomical discussions and pictures. The medical recommendations for drug use and surgical intervention run counter to the conservative approach provided by a rehabilitation-oriented chiropractor.
|
|
|
Anatomy of the Shoulder
The shoulder is an elegant piece of machinery. It has the greatest range of motion of any joint in the body. However, this large range of motion can lead to joint problems. Understanding how the different layers of the shoulder are built and connected can help you understand how the shoulder works, how it can be injured, and how challenging recovery can be when the shoulder is injured. The deepest layer of the shoulder includes the bones and the joints. The next layer is made up of the ligaments of the joint capsule. The tendons and the muscles come next.
|
|
|
Acromioclavicular Joint Separation
A shoulder separation is a fairly common injury, especially in certain sports. Most shoulder separations are actually injuries to the acromioclavicular (AC) joint. The AC joint is the connection between the scapula (shoulder blade) and the clavicle (collarbone). Shoulder dislocations and AC joint separations are often mistaken for each other. But they are very different injuries.
|
|
|
Adhesive Capsulitis
Adhesive capsulitis, also called frozen shoulder, is a painful condition. It results in a severe loss of motion in the shoulder. It may follow an injury, or it may arise gradually with no injury or warning.
|
|
|
Biceps Tendonitis
Biceps tendonitis, also called bicipital tendonitis, is inflammation in the main tendon that attaches the top of the biceps muscle to the shoulder. The most common cause is overuse from certain types of work or sports activities. Biceps tendonitis may develop gradually from the effects of wear and tear, or it can happen suddenly from a direct injury. The tendon may also become inflamed in response to other problems in the shoulder, such as rotator cuff tears, impingement, or instability (described below).
|
|
|
Impingement Syndrome
Many people refer to any pain in the shoulder as bursitis. The term bursitis really only means that the part of the shoulder called the bursa is inflamed. Tendonitis is when a tendon gets inflamed. This can be another source of pain in the shoulder. Many different problems can cause inflammation of the bursa or tendons. Impingement syndrome is one of those problems. Impingement syndrome occurs when the rotator cuff tendons rub against the roof of the shoulder, the acromion.
|
|
|
Rotator Cuff Tears
The rotator cuff tendons are key to the healthy functioning of the shoulder. They are subject to a lot of wear and tear, or degeneration, as we use our arms. Tearing of the rotator cuff tendons is an especially painful injury. A torn rotator cuff creates a very weak shoulder. Most of the time patients with torn rotator cuffs are in late middle age. But rotator cuffs tears can happen at any age.
|
|
|
Thoracic Outlet Syndrome
Thoracic Outlet Syndrome causes pain along the top of the clavicle and shoulder. The pain may spread along the inside edge of the arm. Occasionally pain spreads into the hand, mostly into the ring and pinky fingers. Numbness and tingling, called paresthesia, may accompany the pain, especially in the early hours of the morning before it's time to wake up. Symptoms tend to get worse when driving, lifting, carrying, and writing. The arms may also feel tired when held overhead, as when using a blow dryer. It may be harder to hold and grip things, and the hand may feel clumsy.
|
|
|
|
| |
| |
|
| |
|
Primary Shoulder Resources
|
|
|
|
| |
| |
|
| |
|
|
Passive Range of Motion Testing and Post-isometric Relaxation of the Shoulder
By Frank M. Painter, D.C.
Passive range of motion (ROM) testing of the shoulder is accomplished with the patient supine, and the shoulder joint slightly off the table. The humerus should be abducted to 90° away from the body, so that full internal and external rotation of the humerus can be explored. From the neutral position (with the forearm pointing at the ceiling) normal ROM findings would involve a full 90° of external and internal rotation.
|
|
|
Shoulder Girdle Injuries
Chapter 22: “Chiropractic Management of Sports and Recreational Injuries”
By Richard C. Schafer, D.C., FICC and the ACAPress
This chapter concerns injuries of and about the scapula, clavicle, and shoulder. In sports, the shoulder girdle is a common site of minor injury and a not infrequent site of serious disability. It is second only to the knee as a chronic site of prolonged disability. Upper limb injuries amount to about 20% of sport-related injuries. They can be highly debilitating, require considerable lost field time, and can easily ruin a promising sports career.
|
|
|
The Shoulder and Arm
Chapter 7: “Clinical Chiropractic: Upper Body Complaints”
By Richard C. Schafer, D.C., FICC and the ACAPress
Shoulder pain can be deceiving. As in so many musculoskeletal disorders, consideration of pain in the shoulder should not give priority to sudden trauma whether it be of intrinsic or extrinsic origin. Thorough investigation of the history may reveal that trauma did not initiate the first attack or that an injury was just a precipitating event that revealed an underlying degenerative disorder. Besides trauma, shoulder pain may have an inflammatory, a neurologic, a psychologic, a vascular, a metabolic, a neoplastic, a degenerative, a congenital, an autoimmune, or a toxic origin. See Table 7.1.
|
|
|
Shoulder Girdle Trauma
Chapter 16: “The Rehabilitation Monograph Series”
By Richard C. Schafer, D.C., FICC and the ACAPress
The articulations of the scapula, clavicle, and the humerus function as a biomechanical unit. Only when certain multiple segments are completely fixed can these parts possibly function independently in mechanical roles. Forces generated from or on one of the three segments influence the other two segments. Thus, they will be described here as a functional unit. Please underscore this point in your mind as you read this paper.
|
|
|
Joint Trauma
Chapter 8: “The Rehabilitation Monograph Series”
By Richard C. Schafer, D.C., FICC and the ACAPress
The general stability of synovial joints is established by action of surrounding muscles. Excessive joint stress results in strained muscles and tendons and sprained or ruptured ligaments and capsules. When stress is chronic, degenerative changes occur.
|
|
|
Fundamentals of Initial Case Management Following Trauma
Chapter 2: “The Rehabilitation Monograph Series”
By Richard C. Schafer, D.C., FICC and the ACAPress
Without a doubt, no other health-care approach equals the efficacy of chiropractic in the general field of conservative neuromusculoskeletal rehabilitation. For many centuries, therapeutic rehabilitation was a product of personal experience passed on from clinician to clinician. In the last 20 years, however, it has become an applied science. In its application, of course, much empiricism remains that can be called an intuitive art --and this is true for all forms of professional health care.
|
|
|
Chiropractic Management of Upper Extremity Pain (PDF)
Council on Chiropractic Guidelines and Practice Parameters ~ Clinical Synthesis
This 131 page document is a systematic summary of evidence on the effectiveness of chiropractic management for upper extremity and related disorders, including their quantity, quality and summary of conclusions.
|

Return to the LINKS
Since 12–08–2004
Updated 6-11-2023
|
|
|
|
|