

Expectations Influence Treatment Outcomes in Patients with Low Back Pain.
A Secondary Analysis of Data from a Randomized Clinical TrialThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: European Journal of Pain 2019 (Aug); 23 (7): 1378–1389 ~ FULL TEXT
OPEN ACCESS Andreas Eklund, Diana De Carvalho, Isabelle Pagé, Arnold Wong, Melker S. Johansson, Katherine A. Pohlman, Jan Hartvigsen, Michael Swain
Unit of Intervention and Implementation Research for Worker Health,
The Institute of Environmental Medicine, Karolinska Institutet,
Stockholm, Sweden.BACKGROUND: Low back pain (LBP) is a global public health challenge, which causes high health-care costs and the highest burden on society in terms of years lived with disability. While patient expectations for improvement may have effects on LBP treatment outcomes, it remains unclear if psychological profiles modify this relationship. Therefore, the objectives of this study were to investigate if (1) patient expectations predicted short-term outcome, and (2) psychological profile, pain intensity, and self-rated health modified the relationship between expectations and outcome.
METHODS: Data were collected between April 2012 and January 2016 during the inclusion into a randomized controlled trial. Potentially eligible participants were identified through 40 chiropractic clinics located across Sweden. Patient expectations, psychological profile, pain intensity, activity limitation, and self-rated health were collected from patients with recurrent persistent LBP during their first chiropractic visit (n=593). Subjective improvement was measured at the fourth visit.
RESULTS: Patients with a high expectation of improvement had 58% higher risk to report an improvement at the fourth visit (RR=1.58, 95% CI: 1.28, 1.95). Controlling for potential confounders only slightly decreased the strength of this association (RR=1.49, 95% CI: 1.20, 1.86). Baseline pain intensity, psychological profile, and self-rated health did not modify the effect of expectation on outcome.
CONCLUSIONS: Baseline patient expectations play an important role when predicting LBP treatment outcomes. Clinicians should consider and address patient expectations at the first visit to best inform prognosis.
Significance This study confirms the importance of patient expectations in a clinical setting. Patient expectations predicts the short-term outcome of chiropractic care for LBP. Pain intensity, psychological profile and self-rated health did not modify this relationship.
From the FULL TEXT Article:
Introduction
Low back pain (LBP) is a global health challenge that researchers and policy makers need to face [Buchbinder, van Tulder et al. 2018, Clark and Horton 2018, Hartvigsen, Hancock et al. 2018]. With high prevalence [Vassilaki and Hurwitz 2014], recurrence rates [Von Korff and Saunders 1996, Pengel, Herbert et al. 2003], and health-care costs [Ekman, Johnell et al. 2005, Haldeman, Kopansky-Giles et al. 2012], LBP places the highest burden on society in terms of years lived with disability [Hoy, March et al. 2014]. LBP is not only a societal problem, it also has profound impacts on an individual level with both psychological and social consequences [MacNeela, Doyle et al. 2015]. The condition is still poorly managed clinically with limited use of recommended first-line treatments and inappropriately high use of imaging, rest, opioids, spinal injections, and surgery [Foster, Anema et al. 2018]. Since over 90% of LBP cases have no underlying spinal pathology or other specific disease causing their pain (i.e., no structural diagnosis can be made) [Krismer and Van Tulder 2007], the target for clinical intervention in non-specific LBP cannot be identified from a biomedical perspective [Friedly, Standaert et al. 2010]. The biopsychosocial model, where physical/biological and psychosocial factors are addressed during care, recognizes that patient expectations regarding treatment outcomes, recovery time, and expectations of improvements about their pain may influence symptom progression and resolution. Indeed, many studies have found that optimistic patient expectations play a role in treatment outcomes for both acute [Mondloch, Cole et al. 2001, Bishop, Bialosky et al. 2011] and persistent LBP [Gross and Battie 2005, Boersma and Linton 2006]. Further, patients with optimistic expectations are more likely to experience improved treatment outcomes [Kamper, Kongsted et al. 2015], better self-report functional scores [Myers, Phillips et al. 2008], earlier return to work, and less disability claims than those with low expectations [Kapoor, Shaw et al. 2006, Petersen, Larsen et al. 2007, Ebrahim, Malachowski et al. 2015, Opsommer, Rivier et al. 2017].
To improve communication and better support patient-centred care, it is important to effectively manage patient expectations, which are influenced by past experiences with back pain, age, sex, demographical factors, education level, depression, and fear [Goldstein, Morgenstern et al. 2002, Goossens, Vlaeyen et al. 2005, Gepstein, Arinzon et al. 2006, Ozegovic, Carroll et al. 2009, Kongsted, Vach et al. 2014]. Past experiences are usually captured via so called “yellow flags”, some of which assesses modifiable psychological risk factors that are important for assessing chronicity risk and response to treatment [Nicholas, Linton et al. 2011]. In fact, a systematic review including 37 studies found that psychological variables are related to both the onset and progression of back pain from acute to sub-acute and chronic stages [Linton 2000]. While evidence shows that both positive expectations and psychological factors are related to better prognosis overall, it remains unclear whether the relationship between expectations and outcome of treatment holds true for sub-groups of patients with different psychological profiles, different pain intensities, and/or different perceptions of their overall health.
Therefore, the goal of this study was to investigate the impacts of patient expectations on short-term subjective improvement of LBP in patients with recurrent/persistent LBP seeking care from chiropractors. Specifically, our objectives were to investigate whether: (1) patient expectations for improvement predicted short-term subjective improvement (at the fourth visit), and (2) psychological profile, pain intensity and self-rated health modified the relationship between patients’ expectations and outcome (Supporting Figure 1).
METHODS
Scientific review and ethical approval for this longitudinal multicentre study was approved by local ethics committee at Karolinska Institutet (2007/1458-31/4).
Study design, setting and participants
We conducted a secondary data analysis of data collected between April 2012 and January 2016 during the inclusion process of a randomized controlled trial (RCT), prior to the random allocation of participants [Eklund et al., 2014, 2018]. The RCT was designed to investigate a manual therapy intervention (chiropractic maintenance care) aimed at secondary or tertiary prevention of LBP using prescheduled treatments compared to a control group receiving treatment only when the patient experienced a symptomatic need/relapse of pain. In the maintenance care group, patient visits were scheduled at 1–3 month intervals based on the clinical presentation. In the control group, patients were instructed to seek care if their symptoms returned and were treated with frequent visits until again ready to discontinue care. For both groups, treatment content and frequency of visits were tailored according to patient needs as the clinician would do in their usual practice. The data for our present study were collected during the inclusion visit of the RCT, which was designed as an initial treatment phase. Hence, participants in the current study were not yet allocated to a treatment group, but rather were observed as a clinical cohort during the period prior to randomization. This served the purpose of identifying participants eligible for inclusion in the RCT who had experienced definite improvement in LBP after a short-course of care.
Potentially eligible participants were identified through 40 chiropractic clinics located across Sweden. Patients eligible for inclusion were aged from 18 to 65 years, with recurrent (i.e., more than one episode in the past 12 months) and persistent (i.e., more than 30 days of pain in total in the past year) LBP. Exclusion criteria included: patients with pregnancy, serious spinal pathology or prior chiropractic treatment within the last 3 months or patients who did not pay for the treatments themselves. Follow-up time and scheduling of subsequent visits were at the chiropractor's discretion.
Data collection
After providing verbal-informed consent, eligible and consenting participants completed a baseline questionnaire (written consent was provided at a later time point during the randomization visit of the trial), which collected information about sociodemographic factors, current and previous LBP (e.g., intensity and location), comorbid pain (i.e., neck, thoracic), psychological profile, expectations for improvement, self-rated health, general health, type of work (physically demanding), pain medication use and previous visits to a chiropractor. At each consultation, the patients’ treatment responses were systematically recorded by the chiropractor in the patients’ medical charts.
At the fourth visit, patients were asked about their subjective improvement. If a patient reported a “definite improvement” at the second or third visit, the fourth visit follow-up questionnaire was administered at that consultation. Given the pragmatic nature of the follow-ups, the fourth visit occurred at different time points according to the chiropractor's scheduling. No data on the duration of time between visits or the length of the individual treatment period were collected, as this was not part of the primary objective of the trial. Previous research has shown that the fourth visit (for patients seeing chiropractors in the Scandinavian countries) typically occurs within 2 weeks for 42% of the cases, and between 2 and 4 weeks for 29% of the cases [Malmqvist et al., 2008]. The Nordic Subpopulation Program has shown that it is possible to predict long-term outcome, at 3, 6 and 12 months, from a chiropractic treatment program using data collected at the fourth visit [Axen, Jones, et al., 2005; Axen, Rosenbaum, Robech, Larsen, & Leboeuf-Yde, 2005; Leboeuf-Yde et al., 2004; Malmqvist et al., 2008].
Variables and measurementsExposure Patient's expectations for improvement were measured at the first consultation by asking “How likely do you think it is that your back pain will become considerably better?” Possible responses ranged from 0 to 10 on a Numerical Rating Scale (NRS-11), where 0 meant “No chance” and 10 meant “Very likely.” A similar question has been used to assess expectations in relation to recovery [Ekman et al., 2005; Pengel et al., 2003], and return to work [Iles, Davidson, Taylor, & O'Halloran, 2009]. The patients’ expectation data were treated both as a continuous and as a dichotomized variable where a score of 0–5 was considered to reflect “low” expectations and 6–10 was considered as “high” expectations.
Outcome The outcome subjective improvement was measured at the fourth visit using a five-point Likert scale (1 = Definitely worse, 2 = Probably worse, 3 = Unchanged, 4 = Probably improved, 5 = Definitely improved). Patients scoring 1 to 4 were classified as “Not improved” and those answering 5 were classified as “definitely improved.” This cut-point has been deemed clinically significant in previous research [Axen, Jones, et al., 2005; Leboeuf-Yde et al., 2004; Malmqvist et al., 2008], and represents 69.4% of the participants in the current study.
Effect modification variables Psychological profiles were assessed using the Swedish version of the West Haven-Yale Multidimensional Pain Inventory (MPI-S) as part of the baseline questionnaire. This instrument assesses cognitive-behavioural aspects of the patients’ pain experience and classifies patients into three different psychological subgroups. The MPI was developed to assess patients with chronic pain and has been shown to have acceptable reliability and validity [Bergstrom, Bodin, Jensen, Linton, & Nygren, 2001; Bergstrom et al., 1998; Bergstrom, Jensen, Linton, & Nygren, 1999] across a variety of pain conditions such as neck pain and LBP [Bergstrom, Jensen, Hagberg, Busch, & Bergstrom, 2012; Bergstrom, Bergstrom, Hagberg, Bodin, & Jensen, 2010; Turk & Rudy, 1990], temporomandibular disorders [Turk, 1990], headaches [Walter & Brannon, 1991], fibromyalgia [Turk, Okifuji, Sinclair, & Starz, 1996] and cancer pain [Turk et al., 1998]. The instrument has been translated into a number of languages and has been validated across cultures [Flor, Rudy, Birbaumer, Streit, & Schugens, 1990; Lousberg, Schmidt, Groenman, Vendrig, & Dijkman-Caes, 1997; Talo, Forssell, Heikkonen, & Puukka, 2001].
The MPI-S is a 34-item, 8-scales inventory divided into two parts. The first part describes five specific psychological constructs of the pain experience: pain severity, interference, life control, affective distress and support. The second part describes three specific behavioural constructs associated with individuals in close relationships with the patient: punishing responses, solicitous responses and distracting responses. Table S1 describes the scales according to the original article by Kerns et al. [Kerns, Turk, & Rudy, 1985].
In an empirical process, based on the scores from the 8 scales, three different psychological subgroups have been identified [Bergstrom et al., 2001; Everitt, 1993; Turk & Rudy, 1988]. The subgroups have been replicated in several studies and are described as adaptive copers (AC), interpersonally distressed (ID), and dysfunctional (DYS) [Turk, 2005]. Using a straight-forward classification, a sub-procedure in the K-Means algorithm, individuals were classified according to centroid vectors (mean values of the MPI-S scales) for the three MPI-S subgroups AC, ID and DYS that were previously generated when the instrument was translated into Swedish and validated [Bergstrom et al., 2001, 1998, 1999]. For patients with LBP, the MPI-S subgroups have been found to predict treatment outcome [Bergstrom et al., 2012, 1999; Strategier, Chwalisz, Altmaier, Russell, & Lehmann, 1997] and sick leave [Bergström, Hagberg, Bodin, Jensen, & Bergström, 2011; Bergstrom et al., 2010] and are thought to have clinically meaningful properties. Table S2 describes the characteristics of the MPI-S subgroups.
Low back pain intensity was measured at the initial consultation in the baseline questionnaire using a NRS-11, where 0 meant “No pain at all” and 10 meant “Worst imaginable pain.” This method is recommended by experts in back pain research [Dionne et al., 2008], as well as by The National Institutes of Health Task Force on research standards for chronic LBP [Deyo, Dworkin, Amtmann, Andersson, & Borenstein, 2015].
Self-rated health was measured at the initial consultation in the baseline questionnaire using the EuroQol 5 Dimensions questionnaire (EQ5D), a validated instrument with five general health status domains/questions with three response options in each question [Bjork & Norinder, 1999; Brooks, 1996]. By applying population-based preference weights, the score from the instrument is transferred into a scale ranging from 0 to 1 (“health state equal to death” to “health state equal to perfect health”).Statistical analysis
The baseline characteristics of the cohort were described using means with standard deviations (SD), or frequencies with proportions (%). The predictive effect of patients’ expectations for improvement on short-term outcome (i.e., subjective improvement at the fourth visit) was analysed using robust Poisson regression models where the exposure was included both as a continuous as well as a categorical variable as previously described. The magnitude and direction of associations were expressed as relative risks (RR) with corresponding 95% confidence intervals (CI).
The effect modification of psychological profile (MPI-subgroup), pain intensity, and self-rated health (EQ5D) on the relationship between patients’ expectations and outcome (i.e., subjective improvement at fourth visit) was analysed in two steps using robust Poisson regression models. The MPI-S variable was modelled with 3 levels in each regression analysis. These models included patient's expectations and MPI-S subgroups as categorical variables, and MPI-S scales, EQ5D and pain intensity as continuous covariates. Reference groups of patients were arbitrarily chosen for the analysis of categorical predictors. This included participants with low expectations of recovery and participants identified as the adaptive copers MPI-S subgroup for psychological profile.Modelling process Firstly, a univariate regression model between the exposure variable patients’ expectations on the outcome was modelled to investigate the individual association. Secondly, the a priori identified potential effect modifiers (psychological profile, pain intensity, self-rated health) were included in a multivariable regression model using a backward elimination (BE) procedure. Patients’ expectations and effect modification variables were included as both separate variables and interaction terms (to measure effect moderation) in a saturated multiple regression model. Variables with the highest p-value were excluded stepwise one by one until a final model was reached (i.e., based only on variables with a p-value <0.05). The final model was then validated using a bias-corrected bootstrap simulation with 2,000 replications and accelerated confidence intervals. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp, was used for all statistical analyses.
RESULTS

Figure 1

Table 1
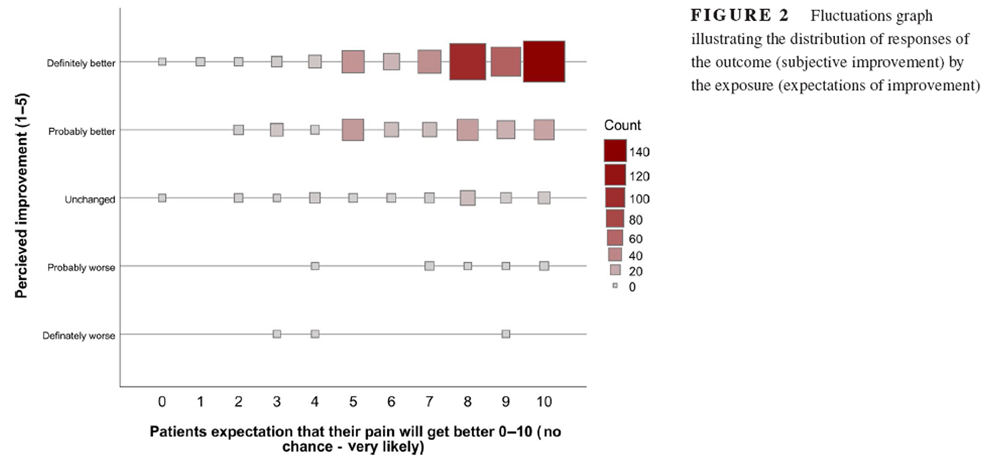
Figure 2
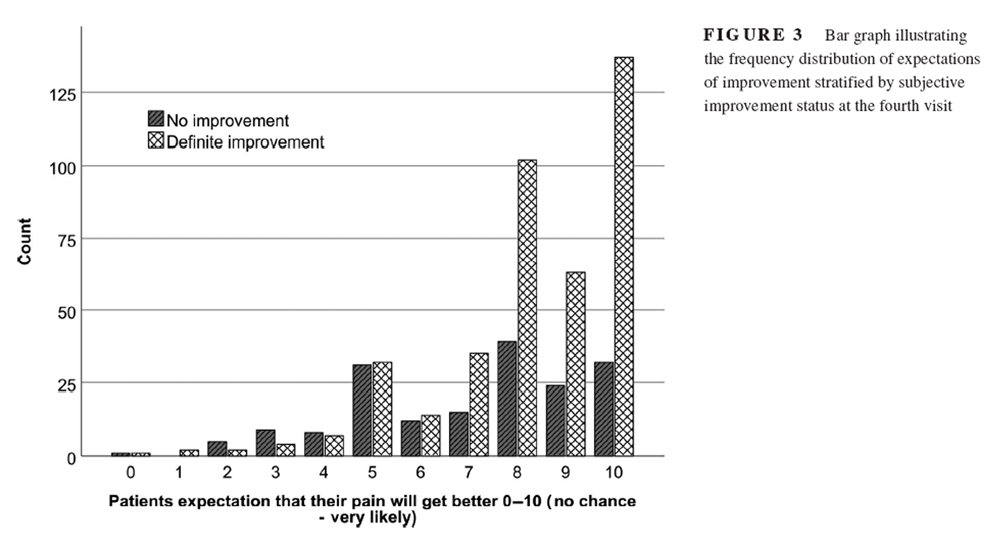
Figure 3
Table 2
Table 3
Table 4 A total of 2,033 patients with LBP were screened for study eligibility. Of those, 1,122 patients did not fulfil the inclusion criteria and were excluded. Out of those 593 participants completed baseline and fourth visit-questionnaires and were included in the analyses (Figure 1). Our study sample consisted of 63.5% women, with a mean age of 43.4 years (the variables sex and age were only available for patients who went on to be included in the clinical trial as these data were collected later, at the final inclusion visit of the RCT). About 60% of LBP patients reported associated leg pain, 66% reported co-occurring pain in the neck or thoracic spine, and 53.7% reported previously visiting a chiropractor for the same problem. Table 1 describes the participant characteristics.
LBP improvement at the fourth visit
Overall 69.4% of participants were “definitely improved” by the fourth visit. The chance of a patient reporting definite improvement by the fourth visit increases on average by 9% for each unit increase on the expectations scale (RR = 1.09, 95% CI: 1.06, 1.13). Figure 2, a fluctuation plot, illustrates the distribution of responses of the outcome (subjective improvement) against the exposure (patients’ expectations). Figure 3 illustrates the number of individuals with a positive or negative outcome for each step on the expectations scale. Among patients who had a high (score of 6–10) versus a low expectation (score of 0–5) of LBP improvement, 74.2% and 47.1%, respectively, reported a definite improvement at the fourth visit. Individuals with a high expectation had 58% higher chance of a definite improvement compared to those having a low expectation (RR = 1.58, 95% CI: 1.28, 1.95).
Effect modification on patients’ expectations and subjective improvement
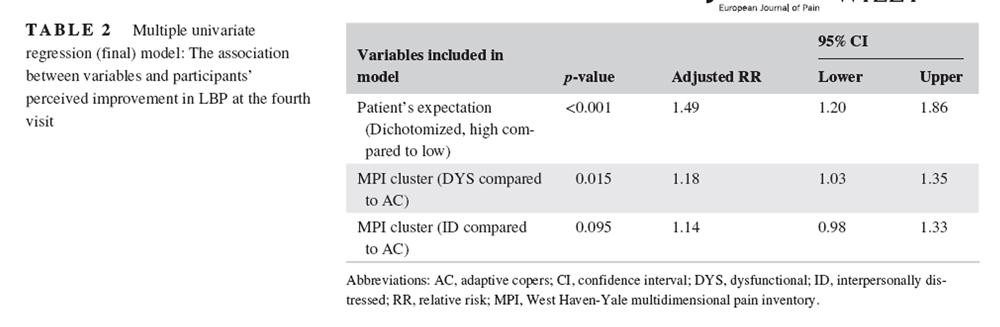
After the BE procedure in the multivariable analysis, only patients’ expectations and MPI-subgroups were left in the final model (Table 2). The addition of a multiple regression model (i.e., controlling for other variables) only slightly decreased the strength of association between patients’ expectations and the outcome (definite improvement at the fourth visit) (from RR = 1.58 to RR = 1.49, as per Table 2). The number of individuals with a positive or negative outcome for each step on the expectations scale for each MPI-S subgroup are reported as supporting information (Figures S2–S4).
In Table 3, we provide the fully saturated model including interaction terms, prior to the backward elimination procedure. The Bootstrap simulation used to validate the final model resulted in almost identical results to the original analysis (Table 4).
Discussion
We have found that patients with high expectations of LBP improvement were more likely to experience improved LBP at the fourth visit, compared to patients with low expectations. In addition to expectations, having a “dysfunctional” psychological profile was also positively associated with LBP improvement at the fourth visit, compared to being an “adaptive coper” and could explain a minor degree of the association between expectations and improvement. However, psychological profile, pain intensity, or self-rated health did not modify the effect between patients’ expectation and LBP improvement.
Previous studies evaluating the associations between recovery expectations, LBP intensity, and subjective improvement are sparse. A 2009 systematic review [Iles, Davidson et al. 2009] looking at recovery expectations to predict LBP outcomes identified expectation as a strong predictor of sick leave and work disability; however, a meta-analysis was not done because of the varying duration of time between the expectation measure and the heterogeneity in outcome measures. Only one of the ten included studies used a 7-point perceived improvement as an outcome measure [Jellema, van der Horst et al. 2006] and none of the included studies were performed in a chiropractic setting, thereby limiting comparison with our results. While some objective outcome measurements (e.g., sick leave) provide important information on LBP recovery, some patients may return to work despite pain. The use of perceived improvement outcome measures provides the opportunity to aggregate all components of LBP patients’ experiences regardless of LBP severity or work disability [Dworkin, Turk et al. 2005]. The current results are in accordance with those of Kongsted et al. [2014] who found that high expectations at baseline were associated with higher probability of improvement three months later in LBP patients seeking care at general practitioners and chiropractic practices [Kongsted, Vach et al. 2014].
Treatment choice may influence patient expectations as indicated by a secondary data analysis from a clinical trial of interventions for neck pain [Bishop, Mintken et al. 2013]. Bishop et al. found that patients unsure of experiencing complete pain relief or improvement in function following spinal manipulative therapy (SMT) had lower odds of reporting a successful outcome compared to patients expecting complete relief after SMT both at one and six months highlighting the importance of patient’s treatment preference. Indeed, not giving SMT to patients who expected that this specific treatment would help them lowered the odds of success. Specific treatment-related expectations were not measured in the current study, but since chiropractors commonly treat back pain patients with SMT [Hurwitz 2012], recovery expectations in our study may have been influenced by patient’s potentially high expectations to receive SMT.
Our data suggest that patients with a less favorable psychological profile have a higher chance of a good short-term treatment outcome compared to the “adaptive coper” subgroup. This finding is unexpected since these psychological profiles have been associated with a higher risk of long term sick leave (dysfunctional and interpersonally distressed) [Bergstrom, Hagberg et al. 2011] and less favorable prognosis (interpersonally distressed) in a multimodal treatment setting [Bergstrom, Jensen et al. 2012]. Possibly this can be explained by a celling effect within the “adaptive coper” sub-group as the room for improvement was greater among the “dysfunctional and interpersonally distressed” sub-groups. It is however noteworthy, that only a minor degree of the association between patient expectations and a successful treatment outcome could be explained by the influence of psychological factors suggesting patient expectations alone is likely to be more relevant from a clinical perspective.
The main strength of the current study is the inclusion of a large sample from a practice-based research network and the use of validated outcome measurement instruments, thus the data should be considered robust and reliable. However, the dichotomization of the expectation variable (score of >5 out of 10 associated to a high expectation) could be considered a limitation as some information is lost and the majority of the data points are in the upper interval of the scale. Although the distribution of data is skewed towards the upper end of the scale, the dichotomization was made at midpoint to avoid classification bias of the true expectation. To address this, the expectation variable was also analysed as a continuous variable in a simple univariate regression model resulting in the same conclusion. Moreover, procedures included in the chiropractic treatment sessions were left to the discretion of the chiropractors and the time-interval between treatment sessions were not controlled or documented. Generalizability to other populations may be limited, as only patients from chiropractic clinics were included. It is not known to which extent these variables could have influenced the results. However, given the pragmatic treatment approaches in the trial and congruency with current literature, our results can be generalized to chiropractic practice.
We believe our study results add to the evidence regarding the value of patients’ expectations of improvement before initiating treatment, as well as propose it might be as important as addressing psychological factors in a clinical setting. These results suggest that expectations for improvement might be a useful prognostic factor; however, the predictive strength of this variable remains to be validated in other settings and cohorts. In the current study, we measured self-perceived improvement as outcome. It is important for future studies to investigate the associations between patient’s expectations and other treatment outcomes to build a comprehensive understanding of the role of expectation in treatment effectiveness in people with LBP. Further, future research can standardize scheduling of visits and the follow-up duration in order to eliminate the variability of this potential confounding variable.
Conclusion
Short-term improvements in patients seeking care from chiropractors for LBP may be influenced by expectations for recovery and this association is not modified by psychological profile, pain intensity or self-rated health. Having a “dysfunctional” psychological profile could, to a minor degree, explain the association between expectations and improvement. However, patient expectations remain the strongest and most clinically relevant predictor for self-perceived LBP improvement. Clinicians should assess their patient’s expectations for improvement at an early stage to identify patients at risk of a poor prognosis.
Acknowledgments
The Chiropractic Academy of Research Leadership (CARL) have been instrumental in this secondary analysis by developing a collaborative structure within the network and through supervision by senior researchers. The statistical support and guidance by Dr. Jan Hagberg have been of great importance for the development of the study’s analytical strategy. The hard-working members of the Swedish Chiropractic Association who collected the data used in the study have greatly contributed to the development of the chiropractic profession and the science base of the field of manual medicine through their participation.
Funding
The original study was funded by the Institute for Chiropractic and Neuro-musculoskeletal Research, the European Chiropractors’ Union (project ID A13.02) and the Danish Chiropractic Research Foundation (grant number 11/148). None of the funding bodies has had any influence of the design, data collection, data analysis, interpretation of the data or in the production of the manuscript.
Conflict of interests
Neither of the authors have any financial or personal conflicts interests so disclose.
References:
Axen I, Jones JJ, Rosenbaum A, Lovgren PW, Halasz L, Larsen K, et al.
The Nordic Back Pain Subpopulation Program: Validation and Improvement of a Predictive Model
for Treatment Outcome in Patients With Low Back Pain Receiving Chiropractic Treatment
J Manipulative Physiol Ther. 2005 (Jul); 28 (6): 381–385Axen I, Rosenbaum A, Robech R, Larsen K, Leboeuf-Yde C.
Can Patient Reactions to the First Chiropractic Treatment Predict Early Favorable Treatment Outcome
in Nonpersistent Low Back Pain?
J Manipulative Physiol Ther. 2002 (Sep); 25 (7): 450–454Bergström, C., J. Hagberg, L. Bodin, I. Jensen and G. Bergström (2011).
Using a psychosocial subgroup assignment to predict sickness absence in a working population
with neck and back pain.
BMC Musculoskelet. Disord. 12(1): 81.Bergstrom, C., I. Jensen, J. Hagberg, H. Busch and G. Bergstrom (2012).
Effectiveness of different interventions using a psychosocial subgroup assignment in chronic
neck and back pain patients: a 10-year follow-up.
Disabil. Rehabil. 34(2): 110-118.Bergstrom, G., C. Bergstrom, J. Hagberg, L. Bodin and I. Jensen (2010).
A 7-year follow-up of multidisciplinary rehabilitation among chronic neck and back pain patients.
Is sick leave outcome dependent on psychologically derived patient groups?
Eur. J. Pain 14(4): 426-433.Bergstrom, G., L. Bodin, I. B. Jensen, S. J. Linton and A. L. Nygren (2001).
Long-term, non-specific spinal pain: reliable and valid subgroups of patients.
Behav. Res. Ther. 39 (1): 75-87.Bergstrom, G., I. B. Jensen, L. Bodin, S. J. Linton, A. L. Nygren and S. G. Carlsson (1998).
Reliability and factor structure of the Multidimensional Pain Inventory--Swedish Language Version (MPI-S).
Pain 75(1): 101-110.Bergstrom, K. G., I. B. Jensen, S. J. Linton and A. L. Nygren (1999).
A psychometric evaluation of the Swedish version of the Multidimensional Pain Inventory (MPI-S):
a gender differentiated evaluation.
European Journal of Pain 3(3): 261-273.Bergstrom, K. G., I. B. Jensen, S. J. Linton and A. L. Nygren (1999).
A psychometric evaluation of the Swedish version of the Multidimensional Pain Inventory (MPI-S):
a gender differentiated evaluation.
Eur. J. Pain 3(3): 261-273.Bishop, M. D., J. E. Bialosky and J. A. Cleland (2011).
Patient Expectations of Benefit from Common Interventions for Low
Back Pain and Effects on Outcome: Secondary Analysis of a
Clinical Trial of Manual Therapy Interventions
J Man Manip Ther. 2011 (Feb); 19 (1): 20–25Bishop, M. D., P. E. Mintken, J. E. Bialosky and J. A. Cleland (2013).
Patient expectations of benefit from interventions for neck pain and resulting influence on outcomes.
J. Orthop. Sports Phys. Ther. 43(7): 457-465.Bjork, S. and A. Norinder (1999).
The weighting exercise for the Swedish version of the EuroQol.
Health Econ. 8(2): 117-126.Boersma, K. and S. J. Linton (2006).
Expectancy, fear and pain in the prediction of chronic pain and disability: A prospective analysis.
European Journal of Pain 10(6): 551-557.Brooks, R. (1996).
EuroQol: the current state of play.
Health Policy 37(1): 53-72.Buchbinder R, van Tulder M, Öberg B, Costa LM, Woolf A, at al.
Low Back Pain: A Call For Action
Lancet. 2018 (Jun 9); 391 (10137): 2384–2388
This is the fourth of 4 articles in the remarkable Lancet Series on Low Back PainClark, S. and R. Horton (2018).
Low Back Pain: A Major Global Challenge
Lancet. 2018 (Jun 9); 391 (10137): 2302
This is the introduction to a 4-article series: The Lancet Series on Low Back PainR.A. Deyo, S.F. Dworkin, D. Amtmann, G. Andersson, et al.,
Report of the NIH Task Force on Research Standards for Chronic Low Back Pain
Journal of Pain 2014 (Jun); 15 (6): 569–585Dionne, C. E., K. M. Dunn, P. R. Croft, A. L. Nachemson, R. Buchbinder, et al. (2008).
A consensus approach toward the standardization of back pain definitions for use in prevalence studies.
Spine 33(1): 95-103.Dworkin, R. H., D. C. Turk, J. T. Farrar, J. A. Haythornthwaite, M. P. Jensen, et al. (2005).
Core outcome measures for chronic pain clinical trials: IMMPACT recommendations.
Pain 113(1-2): 9-19.Ebrahim, S., C. Malachowski, M. Kamal El Din, S. M. Mulla, L. Montoya, S. Bance and J. W. Busse (2015).
Measures of patients' expectations about recovery: a systematic review.
J Occup Rehabil 25(1): 240-255.Eklund A, Axen I, Kongsted A, Lohela-Karlsson M, Leboeuf-Yde C, Jensen I.
Prevention of Low Back Pain: Effect, Cost-effectiveness, and Cost-utility of Maintenance Care -
Study Protocol for a Randomized Clinical Trial
Trials. 2014 (Apr 2); 15: 102Eklund, A., I. Jensen, M. Lohela-Karlsson, J. Hagberg, C. Leboeuf-Yde, et al. (2018).
The Nordic Maintenance Care Program: Effectiveness of Chiropractic Maintenance Care Versus
Symptom-guided Treatment for Recurrent and Persistent Low Back Pain -
A Pragmatic Randomized Controlled Trial
PLoS One. 2018 (Sep 12); 13 (9): e0203029Ekman, M., O. Johnell and L. Lidgren (2005).
The economic cost of low back pain in Sweden in 2001.
Acta Orthop. 76(2): 275-284.Everitt, B. S. (1993).
Cluster Analysis.
London, Arnold.Flor, H., T. E. Rudy, N. Birbaumer, B. Streit and M. M. Schugens (1990).
[The applicability of the West Haven-Yale multidimensional pain inventory in German-speaking countries.
Data on the reliability and validity of the MPI-D.].
Schmerz 4(2): 82-87.Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, et al.
Prevention and Treatment of Low Back Pain:
Evidence, Challenges, and Promising Directions
Lancet. 2018 (Jun 9); 391 (10137): 2368–2383
This is the third of 4 articles in the remarkable Lancet Series on Low Back PainFriedly, J., C. Standaert and L. Chan (2010).
Epidemiology of spine care: the back pain dilemma.
Phys. Med. Rehabil. Clin. N. Am. 21(4): 659-677.Gepstein, R., Z. Arinzon, A. Adunsky and Y. Folman (2006).
Decompression surgery for lumbar spinal stenosis in the elderly:
preoperative expectations and postoperative satisfaction.
Spinal Cord 44(7): 427-431.Goldstein, M. S., H. Morgenstern, E. L. Hurwitz and F. Yu (2002).
The impact of treatment confidence on pain and related disability among patients with low-back pain:
results from the University of California, Los Angeles, low-back pain study.
Spine J 2(6): 391-399; discussion 399-401.Goossens ME, Vlaeyen JW, Hidding A, et al.
Treatment Expectancy Affects the Outcome of Cognitive-Behavioral Interventions in Chronic Pain
Clinical Journal of Pain 2005 (Jan); 21 (1): 18–26Gross, D. P. and M. C. Battie (2005).
Work-related recovery expectations and the prognosis of chronic low back pain within
a workers' compensation setting.
Journal of Occupational and Environmental Medicine 47(4): 428-433.Haldeman, S., D. Kopansky-Giles, E. L. Hurwitz, D. Hoy, W. Mark Erwin, et al. (2012).
Advancements in the Management of Spine Disorders
Best Pract Res Clin Rheumatol. 2012 (Apr); 26 (2): 263–280Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, Hoy D, Karppinen J et al.
What Low Back Pain Is and Why We Need to Pay Attention
Lancet. 2018 (Jun 9); 391 (10137): 2356–2367
This is the second of 4 articles in the remarkable Lancet Series on Low Back PainHoy, D., L. March, P. Brooks, F. Blyth, A. Woolf, et al. (2014).
The Global Burden of Low Back Pain: Estimates from the Global Burden of Disease 2010 study
Ann Rheum Dis. 2014 (Jun); 73 (6): 968–974Hurwitz, E. L. (2012).
Epidemiology: Spinal Manipulation Utilization
J Electromyogr Kinesiol. 2012 (Oct); 22 (5): 648–654Iles, R. A., M. Davidson, N. F. Taylor and P. O'Halloran (2009).
Systematic review of the ability of recovery expectations to predict outcomes
in non-chronic non-specific low back pain.
J. Occup. Rehabil. 19(1): 25-40.Jellema, P., H. E. van der Horst, J. W. S. Vlaeyen, W. A. B. Stalman, L. M. Bouter (2006).
Predictors of outcome in patients with (sub)acute low back pain differ across treatment groups.
Spine 31(15): 1699-1705.Kamper, S. J., A. Kongsted, T. M. Haanstra and L. Hestbaek (2015).
Do recovery expectations change over time?
European Spine Journal 24(2): 218-226.Kapoor, S., W. S. Shaw, G. Pransky and W. Patterson (2006).
Initial patient and clinician expectations of return to work after acute onset of work-related low back pain.
Journal of Occupational and Environmental Medicine 48(11): 1173-1180.Kerns, R. D., D. C. Turk and T. E. Rudy (1985).
The West Haven-Yale Multidimensional Pain Inventory (WHYMPI).
Pain 23(4): 345-356.Kongsted, A., Vach, W., Axř, M., Bech, R.N., Hestbaek, L., Kongsted, A. (2014).
Expectation of Recovery from Low Back Pain: A Longitudinal Cohort
Study Investigating Patient Characteristics Related to Expectations
and the Association Between Expectations and 3-month Outcome
Spine (Phila Pa 1976). 2014 (Jan 1); 39 (1): 81–90Krismer, M. and M. Van Tulder (2007).
Low Back Pain Group of the Bone and Joint Health Strategies for Europe Project.
Strategies for prevention and management of musculoskeletal conditions ….
Best Pract. Res. Clin. Rheumatol.Leboeuf-Yde C, Gronstvedt A, Borge JA, Lothe J, Magnesen E, Nilsson O, et al.
The Nordic Back Pain Subpopulation Program: Demographic and Clinical Predictors for Outcome
in Patients Receiving Chiropractic Treatment for Persistent Low–Back Pain
J Manipulative Physiol Ther. 2004 (Oct); 27 (8): 493–502Linton, S. J. (2000).
A review of psychological risk factors in back and neck pain.
Spine (Phila Pa 1976) 25(9): 1148-1156.Lousberg, R., A. J. Schmidt, N. H. Groenman, L. Vendrig and C. I. Dijkman-Caes (1997).
Validating the MPI-DLV using experience sampling data.
J. Behav. Med. 20(2): 195-206.MacNeela, P., C. Doyle, D. O'Gorman, N. Ruane and B. E. McGuire (2015).
Experiences of chronic low back pain: a meta-ethnography of qualitative research.
Health Psychology Review 9(1): 63-82.Malmqvist S, LeBoeuf-Yde C, Ahola T, Andersson O, Ekström K, Pekkarinen H, Turpeinen M, Wedderkopp N:
The Nordic Back Pain Subpopulation Program:
Predicting Outcome Among Chiropractic Patients in Finland
Chiropractic & Osteopathy 2008 (Nov 7); 16: 13Mondloch, M. V., D. C. Cole and J. W. Frank (2001).
Does how you do depend on how you think you'll do? A systemic review of the evidence for a relation
between patients' recovery expectations and health outcomes (vol 165, 174, 2001).
Canadian Medical Association Journal 165(10): 1303-1303.Myers SS, Phillips RS, Davis RB, Cherkin DC, Legedza A,
Kaptchuk TJ, Hrbek A, Buring JE, Post D, Connelly MT, Eisenberg DM.
Patient Expectations as Predictors of Outcome in Patients with Acute Low Back Pain
Journal of General Internal Medicine 2008 (Feb); 23 (2): 148–153Nicholas, M. K., S. J. Linton, P. J. Watson, C. J. Main and D. F. W. Grp (2011).
Early Identification and Management of Psychological Risk Factors
("Yellow Flags") in Patients With Low Back Pain: A Reappraisal.
Physical Therapy 91(5): 737-753.Opsommer, E., G. Rivier, G. Crombez and R. Hilfiker (2017).
The predictive value of subsets of the Orebro Musculoskeletal Pain Screening Questionnaire for
return to work in chronic low back pain.
Eur J Phys Rehabil Med 53(3): 359-365.Ozegovic, D., L. J. Carroll and J. D. Cassidy (2009).
Does expecting mean achieving? The association between expecting to return to work and recovery
in whiplash associated disorders: a population-based prospective cohort study.
European Spine Journal 18(6): 893-899.Pengel, L. H. M., R. D. Herbert, C. G. Maher and K. M. Refshauge (2003).
Acute low back pain: systematic review of its prognosis.
BMJ 327(7410): 323.Petersen, T., K. Larsen and S. Jacobsen (2007).
One-year follow-up comparison of the effectiveness of McKenzie treatment and strengthening training
for patients with chronic low back pain: outcome and prognostic factors.
Spine (Phila Pa 1976) 32(26): 2948-2956.Strategier, L. D., K. Chwalisz, E. M. Altmaier, D. W. Russell and T. R. Lehmann (1997).
Multidimensional assessment of chronic low back pain: Predicting treatment outcomes.
J. Clin. Psychol. Med. Settings 4(1): 91-110.Talo, S., H. Forssell, S. Heikkonen and P. Puukka (2001).
Integrative group therapy outcome related to psychosocial characteristics in patients with chronic pain.
Int. J. Rehabil. Res. 24(1): 25-33.Turk, D. C. (1990).
Strategies for classifying chronic orofacial pain patients.
Anesth. Prog. 37(2-3): 155-160.Turk, D. C. (2005).
The potential of treatment matching for subgroups of patients with chronic pain:
lumping versus splitting.
Clin. J. Pain 21(1): 44-55; discussion 69-72.Turk, D. C., A. Okifuji, J. D. Sinclair and T. W. Starz (1996).
Pain, disability, and physical functioning in subgroups of patients with fibromyalgia.
J. Rheumatol. 23(7): 1255-1262.Turk, D. C. and T. E. Rudy (1988).
Toward an empirically derived taxonomy of chronic pain patients:
integration of psychological assessment data.
Consult. Clin. Psychol. 56(2): 233-238.Turk, D. C. and T. E. Rudy (1990).
The robustness of an empirically derived taxonomy of chronic pain patients.
Pain 43(1): 27-35.Turk, D. C., T. C. Sist, A. Okifuji, M. F. Miner, G. Florio, et al. (1998).
Adaptation to metastatic cancer pain, regional/local cancer pain and non-cancer pain:
role of psychological and behavioral factors.
Pain 74(2-3): 247-256.Vassilaki, M. and E. L. Hurwitz (2014).
Insights in public health: perspectives on pain in the low back and neck:
global burden, epidemiology, and management.
Hawaii J. Med. Public Health 73(4): 122-126.Von Korff, M. and K. Saunders (1996).
The course of back pain in primary care.
Spine 21(24): 2833-2837; discussion 2838-2839.Walter, L. and L. Brannon (1991).
A cluster analysis of the multidimensional pain inventory.
Headache 31(7): 476-479.
Return to LOW BACK PAIN
Return to SPINAL PAIN MANAGEMENT
Since 4-30-2019


| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |