

Antioxidants and Cancer III: Quercetin This section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Alternative Medicine Review 2000 (Jun); 5 (3): 196–204 ~ FULL TEXT
Davis W. Lamson, MS, ND and Matthew S. Brignall, NDQuercetin is a flavonoid molecule ubiquitous in nature. A number of its actions make it a potential anti-cancer agent, including cell cycle regulation, interaction with type II estrogen binding sites, and tyrosine kinase inhibition. Quercetin appears to be associated with little toxicity when administered orally or intravenously. Much in vitro and some preliminary animal and human data indicate quercetin inhibits tumor growth. More research is needed to elucidate the absorption of oral doses and the magnitude of the anti-cancer effect.
From the FULL TEXT Article:
Introduction
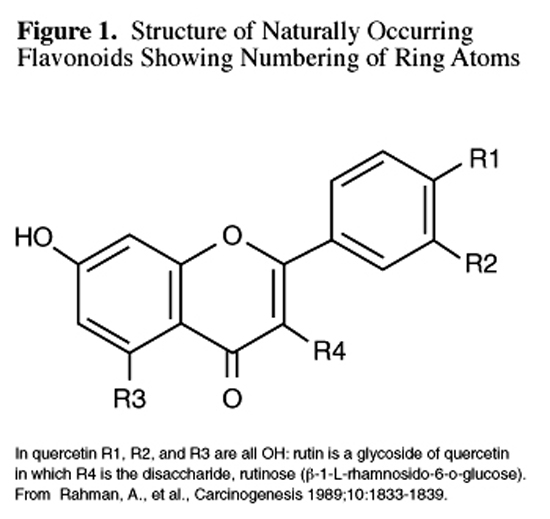
Figure 1 Quercetin (3,3',4',5,7-pentahydroxyflavone; Figure 1, R= OH) belongs to an extensive class of polyphenolic flavonoid compounds almost ubiquitous in plants and plant food sources. Frequently quercetin occurs as glycosides (sugar derivatives); e.g., rutin (Figure 1) in which the hydrogen of the R-4 hydroxyl group is replaced by a disaccharide. Quercetin is termed the aglycone, or sugarless form of rutin. Two extensive volumes, the proceedings of major meetings on plant flavonoids, presented much of the biological and medical data about quercetin in 1985 and 1987. [1, 2]
Quercetin is the major bioflavonoid in the human diet. The estimated average daily dietary intake of quercetin by an individual in the United States is 25 mg. [3] Its reputation as an antioxidant stems from the reactivity of phenolic compounds with free radical species to form phenoxy radicals which are considerably less reactive. Additionally, one can envision a polyphenolic compound easily oxidizable to a quinoid form (similar to vitamin K) and participating in the redox chemistry of nature.
In recent years, research about quercetin has ranged from considering it potentially carcinogenic to examination of its promise as an anti-cancer agent. Four pressing questions arise. Is additional dietary supplementation safe? Is quercetin absorbed and bioavailable when given orally? Is it active against malignant human cells and could its use be developed? Are additional routes such as intravenous or transdermal safe or more advantageous? It is the object of this review to present evidence about these concerns and outline gaps in the available data which need to be filled in order to determine whether quercetin has an appreciable role in future cancer therapy.
Absorption of Quercetin
Most animal and human trials of oral dosages of quercetin aglycone show absorption in the vicinity of 20 percent. An early trial in rabbits showed 25 percent of a 2-2.5 g oral dose was accountable for in the urine. [4] In light of more recent findings of urinary excretion, this is a questionable result. [5] Rats eating a diet supplemented with 0.2-percent quercetin for three weeks attained a serum concentration of 133 microM, mainly in sulfated and glucuronidated forms. [6] Humans fed fried onions containing quercetin glucosides equivalent to 64 mg of the aglycone form reached a maximum serum concentration of 196 ng/ml (0.6 microM) 2.9 hours after ingestion. The half-life of this dose was 16.8 hours, and significant serum levels were noted up to 48 hours post ingestion. [7]
Nine healthy ileostomy patients, chosen to avoid colon flora breakdown of unabsorbed material, were tested for absorption of various forms of quercetin. They absorbed 24 ± 9 percent of 100 mg pure aglycone, 17 ± 15 percent of rutinoside, and 52 ± 15 percent of glucoside given mixed into a meal. Elimination half-life was measured at 25 hours. [8] These findings were surprising in light of the fact that most absorption was previously thought to be exclusively as aglycone and to occur in the large intestine. [9] These findings were later criticized on the ground that no screening was done to rule out malabsorption in a population assumed to have severe gastrointestinal disease. [10] The researchers defended their model based on the normal serum cholesterol concentrations and absorption of PABA. [8] The same investigators fed nine healthy subjects quercetin glucosides equivalent to 64 mg aglycone from onions, glycosides equivalent to 100 mg aglycone from apples, and pure rutinosides equivalent to 100 mg aglycone. Peak plasma levels of 225 ng/ml (0.8 microM) were reached after the onion meal, 90 ng/ml for the apples, and 80 ng/ml for the rutinoside. Half-life was again found to be about 25 hours. [11] Thus, it can be determined that absorption of dietary quercetin is reasonably generous. It has not been determined whether pharmacologic doses are absorbed proportionally.
Until recently, the absorption of oral quercetin was thought to be poor. This was based on a 1975 report that showed a 4-gram oral dose of quercetin aglycone led to no measurable quercetin in either the plasma or urine of healthy volunteers. [12] This report may be flawed on the grounds that the serum assay was only sensitive to 0.1 mcg/ml, a serum level not much less than that found in other trials. Also, urinary output was used as a primary measure of absorption. Later trials have found intact quercetin urinary excretion is negligible. [5,8]
The serum quercetin concentrations required for anti-cancer activity (upwards of 10 microM, see below) are much higher than those achieved with oral doses in human studies. Since a 100 mg single dose was found to create a serum concentration of 0.8 microM quercetin, [11] one could extrapolate that a 1500 mg daily dose might attain a 10 microM level. The relative long half-life of quercetin may result in even higher serum concentrations. Data from an animal study cited above suggest that concentrations of quercetin above 10 microM are attainable with oral doses. [6] A single intravenous dose in humans of 100 mg led to a serum quercetin concentration of 12 microM (4.1 mcg/ml). [12]
Safety of Quercetin
A single oral dose of up to four grams of quercetin was not associated with side-effects in humans. [12] Single intravenous bolus doses of 100 mg were apparently well tolerated as well. [12] Intravenous bolus of 1400 mg/m2 (approximately 2.5 grams in a 70 kg adult) once weekly for three weeks was associated with renal toxicity in two of ten patients. The two patients had a reduction in glomerular flow rate of nearly 20 percent in the first 24 hours. The reduction resolved within one week, and this effect was not cumulative over subsequent doses in the phase I trial in a population of advanced cancer patients. In one patient, nephrotoxicity was averted on subsequent doses by administration of IV saline before and 5-percent dextrose after quercetin. Transient flushing and pain at the injection site were noted in a dose-dependent manner. The 1400 mg/m2/week dose was recommended for a phase II trial. [13]
Quercetin has long been known to be among the most mutagenic of the flavonoids. This property has been demonstrated in the Ames test, [14] in cell culture, [15] and in human DNA. [16] The urine and feces of rats given oral or intraperitoneal doses of quercetin have been found to have mutagenic activity, suggesting this property may be important in vivo. [17]
Mutagenicity does not always imply carcinogenicity, however. Most studies have found quercetin to have no carcinogenic activity in vivo. An early study found that rats consuming diets containing up to 1-percent quercetin (roughly 400 mg/kg) over 410 days had no increase in gross pathology. Total body weight, as well as organ weights were found to be similar to control animals. No increased risk of cancer was found in quercetin-treated animals compared with controls. [18] A later rat study found diets containing as much as 10- percent quercetin for 850 days caused no significant change in body weight or increase in tumor number or size compared with controls. [19] Administration of diets containing up to 10-percent quercetin to golden hamsters for 735 days was also not found to lead to increased tumor incidence compared to control diets. [20] Other similar studies have found a lack of carcinogenicity of quercetin and its glycosides. [21-23]
There are, however, studies that do appear to show an increased risk of tumors with quercetin administration. In a study by Pamucu et al, albino Norwegian rats were fed a diet supplemented with 0.1-percent quercetin for 406 days. By the conclusion of the experiment, 80 percent of treated rats had developed intestinal tumors and 20 percent had bladder tumors. No tumors of either type were seen in control animals. Mean survival times were similar in treated and untreated animals. [24] It is yet unknown why these results are so vastly different from other published trials. A possible explanation is that the trials where quercetin was not found to be carcinogenic had control diets consisting of commercial pellets, while the Pamukcu study used a grain based control diet. [20] Perhaps the finding of carcinogenicity was specific to the strain of rats (Norwegian), and cannot be generalized to other species. A bimodal curve of carcinogenicity is unlikely, as the trial by Ambrose et al found no increased tumor incidence in rats fed 0.25 percent quercetin as well as higher doses. [18] As yet, the meaning of the findings of Pamukcu et al are not clear, and should be interpreted cautiously.
The National Toxicology Program (NTP) investigated the carcinogenicity of quercetin by feeding F344/N rats diets consisting of up to 4-percent (1900 mg/kg) quercetin for 728 days. An increase of renal tubular adenomas was seen in males in the 4-percent quercetin group compared with controls (8/50 compared with 1/50). This increase was not found in females.3 These data have been criticized on the grounds that the increase in benign tumors was only noted when additional step sections were analyzed, making these findings of unclear significance. [25, 26] The NTP trial also found a dose-related decrease in mammary fibroadenomas in treated animals (9/50 in high-dose compared with 29/50 controls). Other than the renal adenomas, no other lesions were noted related to quercetin. [3] At the present time, quercetin is not classified by the NTP report as a human carcinogen. It is also unclear from the published report if the control animals also underwent the additional step-section analysis.
Major Molecular Mechanisms of Action
Down Regulation of Mutant P53 Protein

Figure 3 Quercetin (248 microM) was found to down regulate expression of mutant p53 protein to nearly undetectable levels in human breast cancer cell lines (Figure 3). Lower concentrations gave less reduction. [27] The inhibition of expression of p53 was found to arrest the cells in the G2-M phase of the cell cycle. This down regulation was found to be much less in cells with an intact p53 gene. [28] Mutations of p53 are among the most common genetic abnormalities in human cancers. [29]
G1 Phase Arrest

Figure 2 The G1 checkpoint controlled by the p53 gene is a major site for the control of cellular proliferation (See Figure 2). Quercetin has been found to arrest human leukemic T-cells in the late G1 phase of the cell cycle. At a 70 microM concentration, 64 percent of cells were in G0/G1 compared with 50 percent in control cultures. [30] This G1 arrest was also seen in gastric cancer cells treated with quercetin. Concentrations of 70 microM were found to reduce DNA replication to 14 percent of control values, leading to a delay of cell division. This effect was reversible upon removal of quercetin from the medium. At the 70 microM concentration, quercetin was found to reduce growth of cell cultures to 10 percent of that seen in controls. [31]
Tyrosine Kinase Inhibition
Tyrosine kinases are a family of proteins located in or near the cell membrane involved in the transduction of growth factor signals to the nucleus. In patients with advanced cancers, intravenous administration of quercetin (dosages 60-1700 mg/m2) led to inhibition of lymphocyte tyrosine kinase at one hour in nine of eleven cases. This inhibition was seen as late as 16 hours post-administration.13 In vitro experiments have confirmed these results, both in non-malignant cells [32] and in rat mammary tumor cells. [33] Tyrosine kinase expression is thought to be involved in oncogenesis via an ability to override normal regulatory growth control. [13,34] Drugs targeting tyrosine kinase activity (tyrphostins) are envisioned as possible antitumor agents without the cytotoxic side-effects seen with conventional chemotherapy. [35] Quercetin was the first tyrosine kinase inhibiting compound tested in a human phase I trial. [13]
Estrogen Receptor Binding Capacity
The role of the type II estrogen receptor (ER II) in vivo is not entirely clear. Although the ER II does bind estrogen in vitro, the low affinity makes it likely these sites are occupied by another ligand. One possible explanation offered is that ER II sites are intended for a flavonoid-like substance with growth-inhibitory capability. [36] Quercetin has been shown to induce ER II expression in both type I estrogen receptor positive (ER+) and type I estrogen receptor negative (ER-) human breast cancer cells. The induction of ER II allows for greater growth inhibition of ER- cells with quercetin treatment. [37] In cultured human melanoma cells, quercetin was found to bind ER II sites with an affinity similar to tamoxifen and diethylstilbestrol. The concentration required for 50-percent growth inhibition for one cell line was lower for quercetin (7 nM) than for tamoxifen (9 nM), otherwise the growth inhibitory activity of the two compounds was similar. [38] ER II sites are found in normal tissue and on many different human tumor types, including breast, ovarian, colorectal, meningeal, leukemic, and melanoma. [38] ER II expression is independent of estrogen-receptor (type I) status.
Inhibition of Heat Shock Proteins
Quercetin has been found to inhibit production of heat shock proteins in several malignant cell lines, including breast cancer, [39] leukemia, [40] and colon cancer. [41] Heat shock proteins form a complex with mutant p53, which allows tumor cells to bypass normal mechanisms of cell cycle arrest. Heat shock proteins also allow for improved cancer cell survival under different bodily stresses (low circulation, fever, etc.), and are associated with shorter disease free survival [42] and chemotherapy drug resistance [43] in breast cancer.
Inhibition of Expression of Ras Proteins
Quercetin (10 microM) has been found to inhibit the expression of the p21-ras oncogene in cultured colon cancer cell lines. [44] Mutations in this important gene usually impair cellular GTP-ase, which has the effect of continual activation of the signal for DNA replication. Mutations of ras proto-oncogenes are found in over 50 percent of colon cancers, as well as many other tumor types. [45]
In Vitro Studies of Quercetin

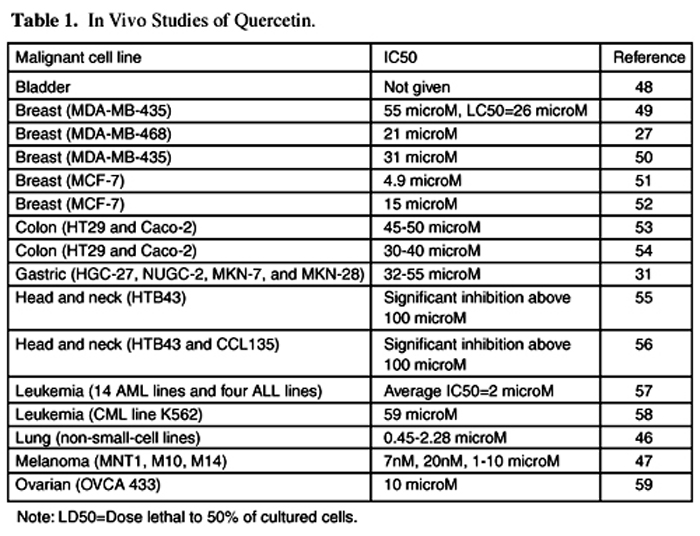
Table 1 Table 1 summarizes the in vitro experiments which have studied the malignant cell culture growth inhibition of quercetin. Each assay showed quercetin to significantly inhibit growth. The quercetin concentration at which tumor cell growth was inhibited by 50 percent inhibitory concentration (IC50) ranged from 7 nM to just over 100 microM. Serum quercetin concentrations of 12 microM have been achieved in humans with single IV doses [12] with no associated side-effects, and up to 400 microM with little toxicity noted. [13] Concentrations of serum quercetin over 100 microM have been attained with oral doses in animal studies. [6]
Two of the assays shown in Table 1 compared the IC50 of quercetin with that of tamoxifen. [46,47] In both cases, the two compounds had similar inhibitory concentrations, which the authors believe reflected their nearly identical affinity for type II estrogen binding sites.
In Vivo Studies of Quercetin
As yet, there has only been one phase I trial of quercetin in advanced cancer patients who were no longer responsive to chemotherapy. The dose escalation and adverse events seen in this trial were discussed above in the toxicity section. Although none of the treated patients met the World Health Organization definition of tumor response (partial response: 50-percent reduction in tumor mass for greater than 30 days), two of 11 patients did have positive results. One hepatocellular carcinoma patient had a sustained (150 days) fall in serum alpha-fetoprotein and alkaline phosphatase during and after four low-dose, intravenous quercetin treatments (60mg/m2) on a 3-week schedule. A patient with stage four ovarian cancer who had not responded to six courses of cyclophosphamide/cisplatin chemotherapy had a fall in the CA125 tumor marker from 290 to 55 units/ml following two treatments of intravenous quercetin (420 mg/m2) three weeks apart. She was continued on this treatment, with less frequent administration and the addition of carboplatin for six months. There was continued suppression of the tumor marker with no mention of tumor size. No data were reported from the other patients. Intravenous quercetin was found to inhibit lymphocyte tyrosine kinase in nine of 11 patients assayed. As is usual in a phase I trial, the focus of the authors was on pharmacokinetics and toxicity, rather than tumor outcome. [13]
Two animal studies have looked at the anti-tumor properties of quercetin. In one study, mice were inoculated with ascites tumor cells and then treated intraperitoneally with either quercetin or its glycoside, rutin. Animals treated daily with 40 mg/kg quercetin had a 20-percent increase in life span, while those treated with 160 mg/kg rutin had a 50-percent increase in life span. If the rutin treatment was split into two 80 mg/kg treatments per day, the increase in life span became 94 percent.60 These in vivo results are interesting since in vitro work showed rutin to have little effect compared to quercetin on tumor tissue. [54,57]
Another animal study looked at the effect of quercetin on mice bearing abdominal tumors derived from a human pharyngeal squamous cell carcinoma line. The mice were given a daily intraperitoneal injection of quercetin. All doses tested (20-, 200-, 400-, and 800 mg/kg) demonstrated significant inhibition of tumor growth. The 20 mg/kg dose had an effect only slightly less than that seen with 800 mg/kg. The effect on the growth of normal human fibroblast cells was minimal. The authors concluded that quercetin appears to be a selective inhibitor of tumor cell growth. [56]
Use of Quercetin with Standard Oncologic Therapeutics
Radiotherapy
An in vitro study showed a significant but mild enhancement of the cytotoxic effect of radiation on rat hepatoma cells when quercetin was added to the medium. [61] A human study showed topical and oral administration of quercetin to reduce skin damage during radiotherapy in patients with head and neck cancers. [62]
Chemotherapy
Quercetin has been shown to increase the therapeutic efficacy of cisplatin both in vivo and in vitro. In mice bearing human tumor xenografts, intraperitoneal treatment with a combination of 20 mg/kg quercetin and 3 mg/kg cisplatin led to a significantly reduced tumor growth compared to treatment with either drug alone. [63] In contrast to the experiment using various doses of quercetin on pharyngeal cancer xenografts in mice discussed above,56 treatment with 20 mg/kg quercetin was not found to be an effective single agent therapy. An in vitro study using human ovarian and endometrial cancer cell lines found that addition of 0.01 to 10 microM quercetin to cisplatin caused 1.5- to 30-fold potentiation of the cytotoxic effect of cisplatin. An absence of potentiation of the effect of adriamycin or etoposide due to quercetin administration was noted. [64] Quercetin (10-100 microM) has also been shown in vitro to protect normal renal tubular cells from cisplatin toxicity. [65]
An in vitro study showed quercetin worked synergistically with busulphan against human leukemia cell lines. Quercetin/busulphan concentrations in 1:1 and 3:1 ratios led to demonstration of much smaller cytotoxic doses of busulphan. [58] Addition of 1-10 microM quercetin to adriamycin treatment led to a dose-dependent increase in cytotoxicity compared with chemotherapy treatment alone in cultured multidrug-resistant human breast cancer cell lines. [66] Quercetin has also been shown in vitro to increase the cytotoxic effect of cyclophosphamide, [67] and to decrease resistance to gemcitabine and topotecan. [68] These last findings are consistent with the fact that many flavonoids have been shown to decrease resistance to chemotherapy in multidrug-resistant tumor cell lines. The mechanism of this action is unclear.
Future Research Directions
At the present time there are considerable in vitro data that support the concept of quercetin as an anti-cancer compound. These promising data have not been followed up with extensive human or animal research. This has left a number of knowledge gaps regarding the use of quercetin as a cancer treatment. These gaps can best be demonstrated by returning to the questions posed in the introduction.
Is Dietary Supplementation of Quercetin Safe?
Human studies have not shown any adverse effects associated with oral administration of quercetin in a single dose of up to four grams12 or after one month of 500 mg twice daily. [69] If quercetin is administered by the intravenous route, it is advised to check kidney function on a regular basis. The question of carcinogenicity of quercetin still merits further exploration, but most data suggest increased cancer risk is not likely associated with oral doses of quercetin.
Is Quercetin Absorbed and Bioavailable When Given Orally?
The absorption studies cited above suggest dietary quercetin is indeed readily taken up in the human intestine. There are many questions here, however. One is whether pharmacological doses are absorbed in the same percentage as dietary concentrations (roughly 20%). A recent experiment demonstrating quercetin to be an effective agent for prostatitis suggests enough quercetin is absorbed from oral megadoses (500 mg twice daily) to have a biological effect, [69] but this has yet to be confirmed in a cancer situation. Another question concerns whether tissue concentrations of quercetin mirror those found in the bloodstream. At least one study has found free serum quercetin to be less than one percent of the total pool, indicating that it is tightly bound to albumin in vivo. These authors hypothesized that very little quercetin is available at the tissue level. [70] A third question concerns whether the conjugated forms of quercetin making up most of the circulating pool6 have similar anti-cancer properties to the aglycone used in most experiments.
Is It Active Against Malignant Human Cells and Could Its Use Be Developed?
Although the in vitro evidence is very strong in this regard, there are cautions. As discussed in the previous paragraph, it is currently unknown if the forms of quercetin most common in human serum (sulfated and glucuronidated) have similar activities to the aglycone. The major question remains whether in vitro research is an accurate model for in vivo systems.
Whether quercetin has any advantageous or detrimental effects on immune function in cancer is an important concern. Quercetin has a history of use by nutritional physicians as an anti-inflammatory and anti-allergy agent.10 This action is thought to be largely due to the inhibition of lipoxygenase and cyclooxygenase, leading to a reduced production of eicosanoid inflammatory mediators. Quercetin is thought to inhibit cyclooxygenase more potently than lipooxygenase. [71] Inhibitors of cyclooxygenase (NSAIDS) are currently under research as potential chemotherapeutic agents, particularly for colon cancer. [72] Cyclooxygenase is known to be elevated in certain epithelial tumors, [73] and is thought to be involved in angiogenesis. [74]
Certain drugs known to decrease eicosanoid production are also known to decrease immune function (e.g., prednisone). Quercetin has been shown in vitro to significantly reduce natural killer cell cytotoxicity at 1 mM, and non-significantly to concentrations as low as 1x10-11 M. [75] However, when rats were fed 100 mg/kg quercetin for seven weeks, they were found to have increased natural killer cell activity compared to those fed placebo. [75] So there appears either an in vitro/in vivo confliction of effect or a biphasic concentration effect. Since the quercetin dose associated with increased immune function is much higher than that usually used in humans, the applicability of this study is questionable.
Are Additional Routes Such as Intravenous or Transdermal Safe or More Advantageous?
Since quercetin is quickly metabolized in the liver, it is very possible that the best means of administration could be those that avoid the first-pass effect. The pilot trial of intravenous dosage gave promising results, and merits follow-up in a larger population. Transdermal use of quercetin has not been explored in humans to date.
Conclusion
In vitro research has shown quercetin to have a number of separate and independent mechanisms of anti-tumor action. Preliminary animal and human studies have confirmed that quercetin does indeed have therapeutic activity in at least some cancer situations. Quercetin has not shown any interference with chemotherapeutic agents to the extent to which it has been studied. Further research will be required to outline the types of malignancy most likely to benefit from this relatively non-toxic therapy. Presently, the oral use of quercetin appears safe and possibly useful in cancer patients.
For more information on antioxidants and cancer, refer to Altern Med Rev 1999;4(5):304-329 and Altern Med Rev 2000;5(2):152-163.
The authors wish to thank Richard Russell and the Smiling Dog Foundation for financial support of this project and to Bastyr University for its administration.

Return to ANTIOXIDANTS
Return to BIOFLAVONOIDS
Return to CANCER AND NUTRITION
Return to CHIROPRACTIC AND CANCER
Since 6-13-2003
| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |