

Does Sedentary Behaviour Cause Spinal Pain in Children
and Adolescents? A Systematic Review With Meta-analysisThis section is compiled by Frank M. Painter, D.C.
Send all comments or additions to: Frankp@chiro.org


FROM: Br J Sports Med 2024 (Oct 22) [EPUB] ~ FULL TEXT
OPEN ACCESS Laura R C Montgomery • Michael Swain • Amabile B Dario • Mary O'Keeffe • Tie P Yamato
Jan Hartvigsen • Simon French • Christopher Williams • Steve Kamper
School of Public Health,
Faculty of Medicine and Health,
The University of Sydney,
Sydney, New South Wales, Australia

Objective: To evaluate whether sedentary behaviour is a risk or prognostic factor for spinal pain in children and adolescents. Specifically, to estimate the (1) direction and strength of the association; (2) risk of spinal pain onset and (3) effect on spinal pain prognosis.
Design: Systematic review with meta-analysis.
Data sources: Electronic searches of MEDLINE, Embase, CINAHL and Web of Science up to 23 March 2023.
Eligibility criteria for selecting studies: Reports estimating the effect of sedentary behaviour on spinal pain in young people ( ≤19 years).
Results: We included 129 reports, 14 were longitudinal (n = 8 433) and 115 were cross-sectional (n > 697 590). We incorporated 86 studies into meta-analyses. (1) From cross-sectional data, we found low certainty evidence of a small positive association between sedentary behaviour and spinal pain (adjusted odds ratio 1.25 (95% CI 1.17 to 1.33), k = 44, n > 92 617). (2) From longitudinal data, we found low certainty evidence of no increased risk for the onset of spinal pain due to sedentary behaviour (adjusted risk ratio 1.07 (95% CI 0.84 to 1.35), k = 4, n = 1 292). (3) No studies assessed prognosis.
Conclusion: Cross-sectional data suggest minimally higher odds of spinal pain for children and adolescents who engage in greater sedentary behaviours. However, longitudinal data do not support a causal relationship, indicating that sedentary behaviour does not increase the risk for onset of spinal pain. Due to the low certainty of evidence, these findings must be interpreted with caution. We found no evidence of the effect sedentary behaviour has on spinal pain prognosis in children and adolescents, highlighting a considerable gap in the literature.
Keywords: Adolescent; Back; Child; Neck; Sedentary Behavior.
WHAT IS ALREADY KNOWN ON THIS TOPIC
The prevalence of spinal pain increases from childhood to adolescence, and previous episodes elevate the risk of adult spinal pain.
In young populations, psychosocial and familial factors are often negatively associated with spinal pain; however, motor performance factors and backpack weight are not linked to spinal pain.
The impact of sedentary behaviour on the risk for onset of spinal pain and its prognosis in children and adolescents remains unclear.
WHAT THIS STUDY ADDS
The relationship between sedentary behaviour and spinal pain in children and adolescents has been extensively estimated in cross-sectional studies (115 reports); however, few longitudinal studies assessed risk of onset (14 reports) and prognosis (0 reports).
Based on low-certainty evidence from meta-analyses of cross-sectional data involving more than 224,862 participants, there are minimally higher odds of spinal pain for children and adolescents who engage in greater sedentary behaviours.
However, from meta-analyses of longitudinal data involving more than 1,292 participants, sedentary behaviour is not a risk factor for the onset of meaningful spinal pain in children and adolescents.
From the Full-Text Article:
Introduction
Rationale
Spinal pain, encompassing discomfort in the neck, mid back or low back, exhibits an increasing prevalence from childhood through adolescence. Nearly 40% of individuals younger than 19 report experiencing spinal pain at least once in their lifetime, with 20% reporting a rise in frequency over time. [1–4] A substantial portion — nearly one-quarter — of children and adolescents experience chronic or recurrent spinal pain that impacts various aspects of their lives, including healthcare and medication use, physical activity, daily functioning, school and work attendance, and overall quality of life. [5–7] Chronic spinal pain can also create financial burden on families and society. [8] Musculoskeletal pain, including spinal pain, has an estimated annual healthcare cost ranging from US$143 to US$41,379 per child or adolescent in 2021. Associated annual costs include patient/family costs (US$287–US$27,972), lost productivity costs (US$124–US$4,671) and societal costs (US$1,095–US$69,351) per child or adolescent. [8] Importantly, adolescent spinal pain strongly predicts its occurrence in adulthood, where low back pain emerges as the leading cause of years lived with disability. [9, 10] The onset of first episodes of spinal pain during childhood or adolescence, therefore, marks a critical stage for prevention and early intervention.
The majority of spinal pain diagnosed in adolescents is considered primary, lacking a discernible pathoanatomical cause and identified mechanism. [11] In young populations, psychosocial and familial factors are often negatively linked to spinal pain, while some biomechanical factors, including motor performance and backpack weight, are not consistently linked to spinal pain in young populations. [3, 12–16] Conversely, evidence for the role of other biomechanical and lifestyle factors, including sedentary behaviour, remains inconsistent. [3, 12, 14] Strong evidence links sedentary behaviour, particularly screen time, to obesity and moderate evidence indicates adverse effects on blood pressure, cholesterol levels, physical fitness, self-rated health, life satisfaction, social behaviour, academic performance and psychological health in young populations. [17–23] As a result, many countries endorse public health guidelines limiting additional (outside school) daily screen time to under two hours; recent updates target sedentary time in classrooms. [24, 25] However, children and adolescents frequently exceed the recommended limits, with adolescents surpassing children in time spent sedentary. [26] This trend of increased sedentary behaviour, along with decreased physical activity, persists from childhood through adolescence. [27, 28]
Popular culture links spinal pain, specifically neck pain, in children and adolescents to sedentary behaviours and screen use, often labelled as ‘text neck’ by clinicians, researchers and the public. [29, 30] Exploration of the mechanisms linking sedentary behaviour and spinal pain, such as direct mechanisms (eg, sustained forward head posture) and indirect mechanisms (eg, increased adiposity, sleep disturbance, poor mental health), have been inconsistent and inconclusive. [28, 31, 32] No existing systematic review has comprehensively explored the link between sedentary behaviour and spinal pain exclusively in children and adolescents. While previous reviews over the last decade touch on this relationship, they vary in scope and quality. Some solely rely on cross-sectional evidence, [33, 34] lack quantitative analysis, [15, 33, 35, 36] encompass a wide range of risk factors, [15, 35] focus on adults [37–39] or exhibit questionable methodological rigour. [34, 40] Understanding the potential association between sedentary behaviour and spinal pain in children and adolescents may help resolve the controversy, provide actionable insights for public health, clinicians and families, establish the quality of available evidence, identify trends and pinpoint targets for future research.
Objectives
We aimed to evaluate whether sedentary behaviour is a risk or prognostic factor for spinal pain in children and adolescents.
Specific objectives were to(1) estimate the direction (ie, protective or not) and strength (ie, magnitude) of the association between sedentary behaviour and spinal pain;
(2) determine if sedentary behaviour increases the risk for onset of the first or recurrent episode of spinal pain and
(3) examine if sedentary behaviour worsens the prognosis of spinal pain in children and adolescents.
Methods
Protocol registration and reporting
Our review protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO 2020 CRD42020148254). Our reporting adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020.41
Eligibility criteriaTypes of studies and population
Peer-reviewed reports were eligible for inclusion where the participant’s mean age was ≤19 years at enrolment, aligning with the WHO defined upper limit of adolescence. [42] We did not limit the minimum age, follow-up period, sample size, participant characteristics or study context/setting (eg, athletes, school children and data registry). Clinical trials with no-care control group data were eligible for inclusion (ie, wait list and no intervention). Trials with a usual-care or active control group were excluded, as were grey literature or unpublished studies, including conference proceedings.
Types of exposure factors
Reports were eligible for inclusion if they measured and reported sedentary behaviour exposure in accordance with the Sedentary Behaviour Research Network definition: sedentary behaviour includes any behaviour while (1) awake, (2) in a seated, lying or reclining posture and (3) with low energy expenditure. [43] Low energy expenditure is classified as less than three metabolic equivalents (METS), including activities such as watching television (TV) (1.0–1.3 METs), playing traditional video or computer games (1.0 METs), reading or studying (1.3 METs), riding in a car (1.3 METs) and sitting playing a musical instrument (2.0–2.5 METs). [44]
Types of outcomes
To be included, reports must have measured spinal pain according to the following definition by the International Association for the Study of Pain: spinal pain is perceived as arising from the vertebral column or its adnexa (ie, muscles, tendons, nerves, bones and joints of the spine). [45] Reports measuring pain as single or multiregional (eg, neck pain, mid and low back pain) or in combination with an adjacent anatomical region (eg, neck and shoulder pain) were eligible for inclusion. We included all measures of spinal pain intensity, frequency and impact. Spinal pain impact may have included absence from school, taking pain medication or seeking healthcare. We excluded reports where the pain was disease or injury related, including but not limited to cancer, juvenile spondyloarthropathy, postsurgical, Scheuermann’s disease, scoliosis, sporting injury, spondylolisthesis or trauma.
Information sources and search strategy
We searched MEDLINE (OvidSP), Embase (OvidSP), CINAHL (EBSCOhost) and Web of Science from inception to 23 March 2023. During April 2023, we conducted manual reference checks and citation tracking on Scopus for all included reports and relevant reviews. We collaborated with an academic librarian with medical systematic review search methodology expertise at the University of Sydney Library to formulate our search strategy, covering key concepts: sedentary behaviour (eg, TV and screen time), spinal pain (eg, backache, low back pain) and children and adolescents (eg, student and teen). We applied no language restrictions. Online supplemental table 1–4Selection process
Records were exported from databases to EndNote for consolidation and deduplication, then remaining records were imported into Covidence and deduplicated again. Covidence software randomly paired two review authors (of LRCM, MS, ABD, MO’K and TPY) to independently screen English records and subsequently evaluate full-text reports against eligibility criteria for inclusion. For non-English records, researchers in the field fluent in the necessary language were engaged to screen. Discrepancies were resolved via discussion between paired review authors, with the involvement of a third review author if necessary.
Data extraction
Two review authors (LRCM and ABD) independently tested data extraction using a Microsoft Excel pilot form. One review author (LRCM) then extracted data for all English reports; a second review author (of MS, ABD, MO’K and TPY) independently cross-checked all extracted data. Researchers who were fluent in the necessary language extracted data for non-English reports. We extracted details including study characteristics, sample details, sedentary behaviour exposure, spinal pain outcomes and statistical methods (see online supplemental table 5). Both adjusted and unadjusted estimates, such as risk (RR), odds (OR) or prevalence ratios (PR), along with variance measures (eg, 95% CI), were extracted as published in original reports. When multiple adjusted models were reported, we extracted the estimate with more potential confounders to reduce the overall risk of residual confounding. Potential confounders were categorised into individual characteristics (eg, age, sex and BMI) and environmental characteristics (eg, family history and socioeconomic status). Data were extracted for all follow-up periods.
Study risk of bias assessment
Two randomly selected review authors (of LRCM, MS, ABD, MO’K and TPY) independently assessed each included report using our modified Quality in Prognosis Studies (QUIPS) tool via Covidence. [46] Researchers fluent in the necessary language applied QUIPS to non-English reports.
Risk of bias (RoB) was assessed across six domains:(1) study participation,
(2) study attrition (longitudinal reports only,
not applicable for cross-sectional reports),
(3) exposure measure,
(4) outcome measure/s,
(5) study confounding and
(6) statistical analysis and reporting.Domains (3), (4) and (5) were modified a priori (see online supplemental table 6). A report received an overall ‘low’ RoB classification if it scored low in four of the six domains, including (5) study confounding. Discrepancies were resolved via discussion between paired review authors, with the involvement of a third review author if necessary.
Synthesis methods and effect measures
We tabulated and synthesised the included reports in alignment with our three review objectives:(1) cross-sectional reports estimating the association between sedentary behaviour and spinal pain;
(2) longitudinal reports with participants free of spinal pain, or adjusted for its presence, at baseline examining baseline sedentary behaviour and risk for onset or recurrence of spinal pain and
(3) longitudinal reports with participants initially experiencing spinal pain, measuring the effect of baseline sedentary behaviour on the persistence of spinal pain or its impact at follow-up.For objectives (2) and (3), we planned a priori to pool the most adjusted estimates, RRs and ORs separately, when ≥2 longitudinal reports demonstrated sufficient clinical and methodological homogeneity. Due to limited data availability, we made a post hoc decision to also pool the unadjusted longitudinal estimates for objectives (2) and (3), as well as the most adjusted and unadjusted cross-sectional estimates, PRs and ORs separately, for objective (1). Inclusion decisions for estimates in meta-analyses adhered to specified criteria (see online supplemental material figure 1), such as selecting the estimate from the report with a lower RoB when two or more reports present estimates on the same sample. Where an estimate required for meta-analyses was not reported, we contacted study authors once to request missing information. If there was no response, the review authors calculated an unadjusted OR with a 95% CI from the information available if possible. Where we could not complete quantitative synthesis, we provided a narrative synthesis.
Statistical methods
We present primary meta-analysis results for each review objective using forest plots and tabulated results for subgroup and sensitivity analyses. Results are reported as the pooled estimate (OR, RR or PR) with 95% CIs. We employed the inverse variance weighted DerSimonian and Laird random effects model with the ‘metan’ command in STATA/IC V.15.1 for Mac (code available in online supplemental material). We assessed heterogeneity in pooled estimates via visual inspection and I2 statistic, categorised as might not be important (<40%), moderate (30%–60%), substantial (50%–90%) or considerable heterogeneity (>75%).
Subgroup and sensitivity analyses
A priori planned subgroup analyses for longitudinal data aimed to explore the impact of screen-based (eg, TV and computer) and non-screen-based (eg, reading a book and passive travel) sedentary behaviours on spinal pain outcomes. We decided post hoc to also run this subgroup analysis in cross-sectional data. Additionally, post hoc, we performed subgroup analyses to investigate the effect of sex (ie, male and female), age (ie, child <13 years and adolescent ≥13 years), spinal pain region (ie, neck, mid-back and low back) and duration of sedentary behaviour exposure in increasing 2 hours/day increments. We performed post hoc sensitivity analyses to assess the effect of overall low RoB on pooled estimates and duration of follow-up (<12 months and >12 months) on longitudinal pooled estimates.
Certainty assessment and reporting bias assessment
Two review authors (LRCM and ABD) independently applied our a priori modified Grading of Recommendations, Assessment, Development and Evaluation framework to assess evidence certainty for each review objective (see online supplemental material table 7). [47–49] We rated evidence certainty as ‘high’, ‘moderate’, ‘low’ or ‘very low’. Starting with ‘high’ confidence, as outlined by Iorio et al 2015 for systematic reviews of prognosis. [48]
We downgraded by one level of certainty for the following:(1) study limitations; if <30% of participants came from reports rated as overall low RoB,
(2) inconsistency; if the pooled estimate showed substantial or considerable heterogeneity (I2 statistic >50%), or there was wide variability across point estimates,
(3) imprecision; if the pooled estimate had excessively wide 95%CIs, or the evidence comprised few studies with small populations and imprecise estimates,
(4) indirectness; if heterogeneity substantially altered the pooled estimate, or limited its applicability and generalisability and
(5) reporting bias; if there was statistical evidence of reporting bias (based on funnel plot and Egger’s test results), or the relationship had not been repeatedly investigated.Where we could pool ≥10 samples, we inspected funnel plots and results of Egger’s test for reporting bias and small study effects.
We upgraded by one level of certainty for(1) a moderate-to-large pooled effect size
(OR >2.5 or equivalent) and
(2) evidence of a exposure-response gradient.Judgement was applied on overall assessment of the criteria, as there is overlap, so to not excessively downgrade. Discrepancies were resolved via discussion between paired review authors, with the involvement of a third review author if necessary.
Equity, diversity and inclusion statement
In our commitment to inclusivity and thoroughness, we imposed no restrictions on participant characteristics (eg, sex, race, culture and socioeconomic status), study context or setting (eg, regional, city, school and athlete) or publication language to encompass data on marginalised groups. We address limitations in evidence representative of marginalised groups and the generalisation of findings in our discussion. Our review team is committed to promoting equity, diversity and inclusion, and this reflects our gender-balanced composition from diverse cultural backgrounds and different career stages, including early (one), mid (three) and senior (five) researchers.
Patient and public involvement
There was no patient or public involvement in this systematic review.
Results
Study selection
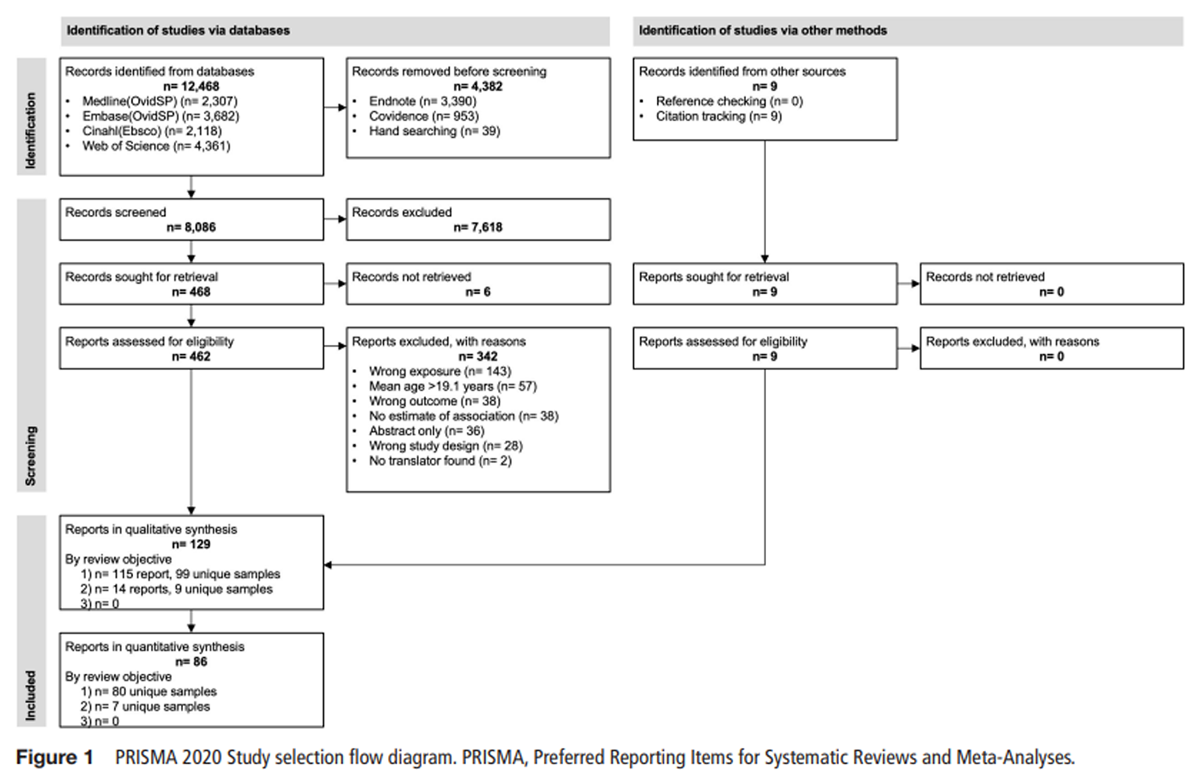
Figure 1 Our searches returned 12,468 records. After screening, we included 129 reports, of which we included 86 studies in meta-analyses (Figure 1). We engaged translators proficient in Chinese, French, German, Korean, Portuguese, Spanish and Turkish to screen abstracts, extract data and assess RoB when required. We excluded one Polish [50] and one Slovenian [51] report due to the unavailability of translators.
Cross-sectional associations: assessing the direction and strength
of the relationship between sedentary behaviour and spinal painStudy selection, characteristics and results of individual studies
We included 115 cross-sectional reports [28, 52–165] covering 99 unique samples, ranging 7–20 years old, and published between 1988 and 2023 (23% in the past 5 years). These studies represent 37 countries, categorised by World Bank income level as 65% high income, 19% upper middle income, 14% lower middle income and 3% low income. [166] Each report, detailed in online supplemental appendix 1 table 1, estimated the direction (ie, protective or not) and strength (ie, magnitude) of the association between sedentary behaviour and spinal pain in children and adolescents.
Risk of bias
Five of the 115 cross-sectional reports had low RoB (overall) (online supplemental appendix 2 table 1). [60, 92, 129, 160, 161] For individual RoB domains, approximately half of the reports received low RoB ratings for study participation (54/115), outcome measurement (60/115) and statistical analysis and reporting (59/115). Fewer reports received low RoB ratings in exposure measurement (3/115) and study confounding (21/115) domains.
Results of syntheses

Table 1
See p. 5Our pooled unadjusted OR of 1.27 (95% CI 1.19 to 1.34, I2 86.9%) included 75 estimates and >118,561 participants. After adjusting for confounders, a similar weak positive association was found in our pooled adjusted OR of 1.25 (95% CI 1.17 to 1.33, I2 88.6%) from 44 estimates and >92,617 participants. Our pooled unadjusted PR of 1.10 (95% CI 1.01 to 1.19, I2 60.6%) included 7 estimates and 7,930 participants. After adjusting for confounders, our pooled adjusted PR of 1.04 (95% CI 0.97 to 1.11, I2 15.3%) included 6 estimates and 5,754 participants. High heterogeneity in pooled estimates was explored in subgroup analyses. There were significant subgroup effects for female sex, age older than 13 years and neck pain. There was no apparent dose–response relationship based on the duration of sedentary behaviour. Sensitivity analysis of reports with overall low RoB remains consistent with our primary meta-analyses. See Table 1, forest plots in online supplemental appendix figure 1a and 2 and the details of the estimate selection process are provided in online supplemental table 8).
Certainty of evidence and reporting bias
Table 2 We found low to very low certainty evidence in cross-sectional associations (Table 2). We downgraded against study limitations, inconsistency and publication bias. Our pooled adjusted and unadjusted ORs had statistical evidence of reporting bias and small study effects. Both funnel plots were asymmetrical, highlighting that studies with smaller effect sizes were missing, and both Egger’s tests had p<0.005 (online supplemental appendix 1 figure 1b,c). We could not inspect for reporting bias in our pooled adjusted and unadjusted PRs.
Longitudinal risk assessment: determining if sedentary
behaviour increases the risk for onset of spinal painStudy selection, characteristics and results of individual studies
Table 3
See p. 7We included 14 longitudinal reports [167–180] covering 9 unique samples, ranging 7–18 years, and published between 2002 and 2023 (36% in the past 5 years). These studies represent 8 countries (75% high-income, 25% upper-middle-income, 0% lower-middle or low-income level) [166] (Table 3).
RoB in studies
Two of the 14 longitudinal reports had low RoB (overall) (online supplemental appendix 2 table 2). [168, 178] The domains with the highest number of low RoB ratings were outcome measurement (11/14) and statistical analysis and reporting (10/14). Approximately half of the reports received low RoB in the study participation and study confounding domains (6/14 each). Only two reports used an objective measure of sedentary behaviour via an accelerometer to achieve low RoB in the exposure measure domain. [167, 168] No report achieved a low RoB rating in the study attrition domain.
Results of quantitative syntheses
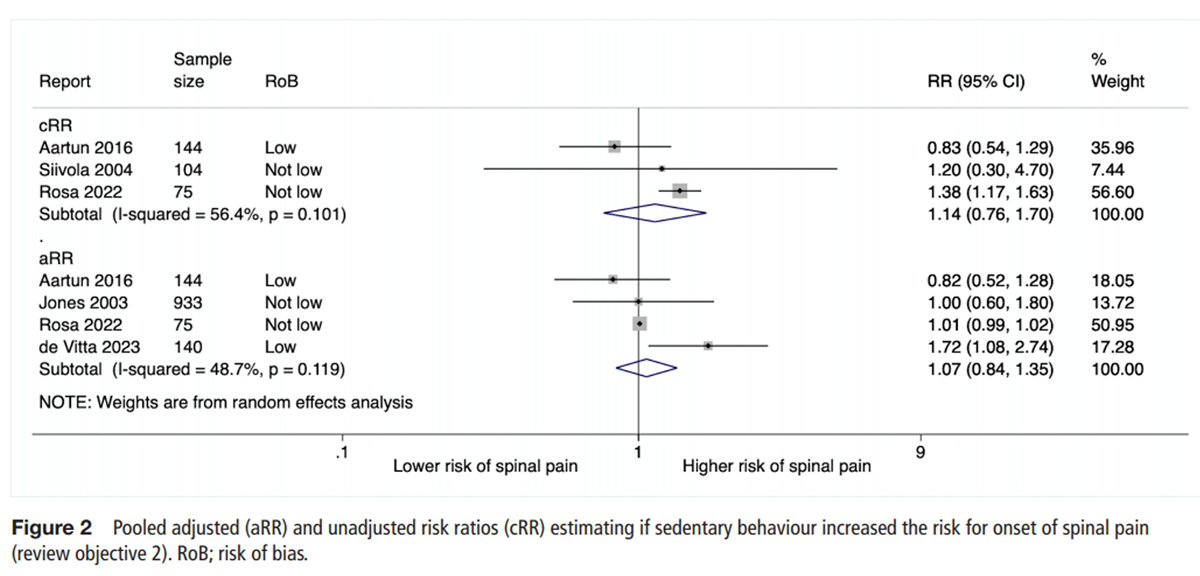
Figure 2
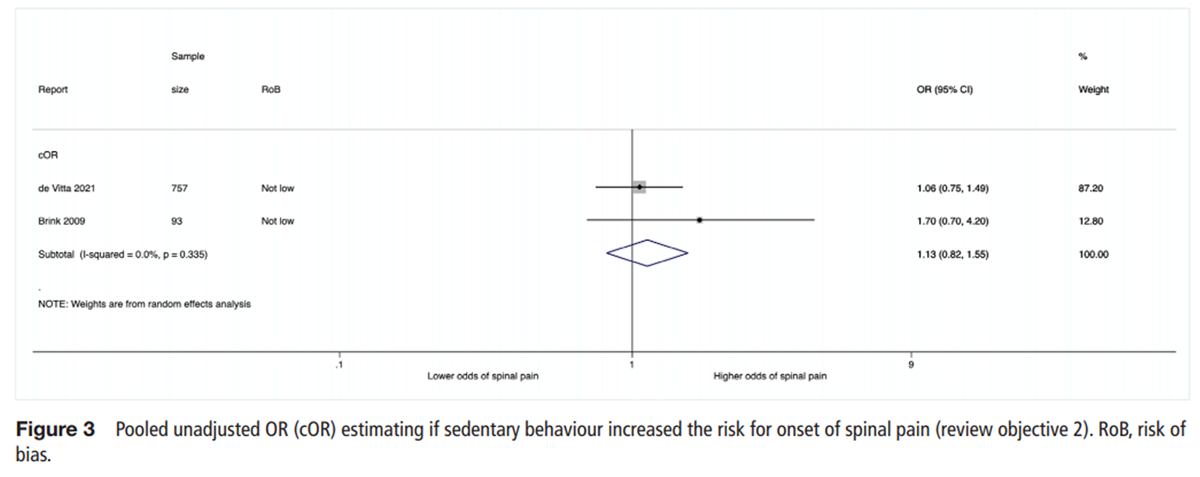
Figure 3 Our pooled unadjusted OR of 1.13 (95% CI 0.82 to 1.55, I2 0%) included 2 estimates with 850 participants. [169, 179] We did not pool an adjusted ORs. Our pooled unadjusted RR of 1.14 (95% CI 0.76 to 1.70, I2 56.4%) included 3 estimates and 323 participants. [168, 171, 175] After adjusting for confounders, we found a similar pooled adjusted RR of 1.07 (95% CI 0.84 to 1.35, I2 48.7%) from 4 estimates and 1,292 participants. [168, 175, 177, 178] Limited data hindered our ability to run subgroup analyses. Our sensitivity analysis of reports with overall low RoB remains consistent with our primary analyses (adjusted RR 1.18 (95% CI 0.57 to 2.45, I2 80.1%) from 2 estimates and 284 participants). See table 1, forest plots in Figures 2 and 3 and the details of the estimate selection process are provided in online supplemental material table 8.
Certainty of evidence and reporting bias
We found low certainty evidence that sedentary behaviour was not a risk factor for the onset of spinal pain in children and adolescents (Table 2). We downgraded due to doubt in publication bias, study limitations and inconsistency. Sedentary behaviour has not been investigated as a risk factor for spinal pain in a large number of longitudinal studies. We could not inspect for statistical evidence of reporting bias.Longitudinal prognosis assessment: evaluating if sedentary
behaviour affects the prognosis of spinal pain
We found no longitudinal reports investigating the effect of sedentary behaviour on the prognosis of spinal pain in children and adolescents.
Discussion
Interpretation
Based on 115 reports, we found that cross-sectional estimates suggest children and adolescents with greater sedentary behaviour have minimally higher odds of spinal pain and no difference in spinal pain prevalence. These associations are unlikely to be causal, as it is equally plausible that children and adolescents with spinal pain tend towards sedentary behaviours. In fact, based on 14 longitudinal reports, our findings indicate sedentary behaviour does not increase the risk for the onset of the first or a recurrent episode of meaningful spinal pain in children and adolescents, regardless of adjustment for potential confounders. These results were consistent in sensitivity analyses, where weak and non-significant associations were found, supporting the robustness of our findings. These review findings should be interpreted cautiously as the evidence is of low certainty and only 11% of the data are longitudinal. We could not identify any evidence of the effect of sedentary behaviour on spinal pain prognosis, highlighting a notable gap in the current literature.
Our cross-sectional analyses aligned with the pooled cross-sectional estimates from Baradaran Mahdavi et al, which showed a weak positive association between sedentary behaviour and neck (unadjusted OR 1.13 (95% CI 0.98 to 1.30)) and low back (unadjusted OR1.20 (95% CI 1.07 to 1.37)) pain in young individuals. [34, 40] Our longitudinal assessment of risk mirrors findings observed in the adult population. Damato et al pooled longitudinal estimates of sedentary behaviour and the risk of low back pain, revealing no association (unadjusted RR 1.01 (95% CI 0.98 to 1.04)). [39] Similarly, both Damato et al and Alzahrani et al investigated whether prolonged sedentary behaviour heightened the risk of low back pain in adults. [38, 39] Their results, consistent with our cross-sectional subgroup analysis, suggested that increased duration of sedentary behaviours did not correlate strongly with increased risk of back pain. No exposure–response relationship was observed between sedentary behaviour and spinal pain. Our results suggest that transient back discomfort felt following prolonged sedentary behaviour is unlikely to progress to meaningful spinal pain in children and adolescents. De Carvalho et al observed the same nuanced relationship in their analysis of objectively measured prolonged sitting in adults. [37] The current evidence does not support the demonising of sedentary behaviours, including screentime, as a cause of meaningful spinal pain in children and adolescents.
Strengths and limitations
The strength of our review includes protocol registration and a thorough search strategy to encompass all existing evidence of the relationship between spinal pain and sedentary behaviour in children and adolescents. Including longitudinal studies allowed us to explore potential causal relationships by examining temporality, specifically that sedentary behaviour preceded spinal pain. However, several limitations warrant consideration. The current evidence base suffers from a scarcity of longitudinal research investigating sedentary behaviour as a risk factor and a complete absence of longitudinal research investigating sedentary behaviour as a prognostic factor for spinal pain in children and adolescents. Additionally, there is an under-representation of lower middle-income or low-income populations, as no longitudinal studies and only 17% of cross-sectional studies represented these populations.
Our confidence in the evidence is low to very low, suggesting the true measure of association or risk may substantially differ from our pooled estimates. This uncertainty stems primarily from the high RoB in included studies, inconsistency in effect estimates across studies and reporting bias. The high RoB and inconsistency in effect estimates may exist due to the majority of studies using subjective measures of sedentary behaviour. Only 5 of 129 reports used objective measures, [52, 72, 118, 167, 168] which are the preferred tool and have the highest validity for measuring physical activity and sedentary time in an adult population. [181, 182] Evidence of reporting bias in cross-sectional data suggests potential under-representation of studies with negative or more negligible positive associations in our pooled estimates. Scarcity of longitudinal data prevented thorough examination of reporting bias. However, had we pooled an adjusted OR, the study by Szpalski et al would have been excluded as the authors noted their estimate was ‘not significant’ and did not report the value. [174] Such reporting practices raise concern that our pooled estimates may be an overestimate of the true effect size.
While heterogeneity in meta-analysis is expected and common, our decision to pool spinal pain and sedentary behaviour data, meeting broad definitions and reporting time frames, may contribute to the high statistical heterogeneity. Nonetheless, we undertook this approach because it provides a more comprehensive synthesis of data and has minimal impact on understanding the impact of sedentary behaviour on spinal pain, clinical or otherwise. Our consistent findings across subgroup and sensitivity analyses suggest that the heterogeneity in our pooled estimates stems from unexamined study characteristics, that is, measures of sedentary behaviour and spinal pain, as discussed above, or potential residual confounding. If a robust association existed, we believe it should withstand scrutiny across heterogeneous populations, exposures and outcomes.
Implications
While reducing sedentary behaviours is important for overall health, it is unlikely to significantly reduce the incidence or lessen the burden of spinal pain in children and adolescents. Clinicians are encouraged to take a balanced approach when discussing sedentary behaviour with children and adolescents experiencing spinal pain. While sedentary behaviour is not a risk factor for clinically meaningful spinal pain, beyond temporary discomfort, it may still be valuable to monitor as part of a comprehensive assessment of overall lifestyle. This may include promotion of healthy habits such as regular physical activity, adequate sleep and addressing psychosocial factors such as stress and mental well-being. There is no evidence yet to inform whether sedentary behaviour affects the persistence (prognosis) of spinal pain, thus when discussing this relationship caution around language use is warranted.
To effectively address spinal pain in young people, it is imperative to identify and address modifiable risk and prognostic factors that have a stronger effect on meaningful or impactful spinal pain. Future research in this field must be more robust, and appropriately designed longitudinal studies are needed to elucidate causal pathways and mechanisms underlying spinal pain. Ideally, prospective cohort studies that objectively capture daily behaviours, measure daily or weekly spinal pain intensity, frequency and impact, and adequately account for relevant confounders. Alternatively, causal inference can be drawn from longitudinal observational research. Given its limitations in establishing causal relationships, further cross-sectional research in this field is unnecessary.
Conclusions
Cross-sectional data suggest a small positive association between sedentary behaviour and spinal pain in children and adolescents. Specifically, our meta-analyses, including over 98 371 participants combined, indicate slightly higher odds of spinal pain among those with greater sedentary behaviours. However, longitudinal data, including 2,465 participants combined, do not support a causal relationship; sedentary behaviour does not appear to increase the risk of developing spinal pain over time in children and adolescents. Given the low certainty of evidence, these findings need to be interpreted with caution. We found no evidence assessing the effect of sedentary behaviour on the prognosis of spinal pain in children and adolescents, highlighting a gap in the literature and area for future research.
Supplementary MaterialSupplemental material 1 Contains OSM Tables 1–8,
Figure 1, and Online Supplementary Material References
Supplemental material 2 Contains Appendix 1 Figure 1 a,
Appendix 1 Figure 2,
Appendix 1 Table 1
Supplemental material 3 Contains Appendix 2 Table 1Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Acknowledgments
The authors would like to acknowledge the methodological expertise of the academic librarians within the Faculty of Medicine and Health, who assisted in developing our search strategy. We also appreciate the statistical assistance provided by the Sydney Informatics Hub, a Core Research Facility of the University of Sydney. We would like to express our gratitude to Emre Ilhan, Wing Kwok, and three other contributors for their invaluable assistance in screening, data extraction, and applying risk of bias assessments to non-English reports.
Contributors
Conceptualisation: LRCM.
Methodology: LRCM, SK, MS, ABD, JH, SF and CW. :
Data searching: LRCM.
Data extraction and RoB application: LRCM, MS, ABD, MO'K, TPY and SK.
Data analysis: LRCM and SK.
Writing (original draft preparation): LRCM.
Writing (review and editing): LRCM, MS, ABD, MO'K, TPY, JH, SF, CW and SK.
Guarantor: LRCM.Funding
LRCM was supported in this research by an Australian Government Research Training Program scholarship and a Chiropractic Australia Research Foundation PhD scholarship.
SK and CW were funded by National Health and Medical Research Council of Australia Fellowships.
References:Refer to FULL Text article
Return to PEDIATRICS
Since 10-29-2024

| Home Page | Visit Our Sponsors | Become a Sponsor |
Please read our DISCLAIMER |